Infectious diseases are prevalent in the world and are one of the world's major sources of morbidity and mortality. Though infectious diseases can initiate in a localized region, they can spread rapidly at any moment due to the ease of traveling from one part of the world to the next. This could lead to a global pandemic. One key to preventing this spread is the development of diagnostics technology that can rapidly identify the infectious agent so that one can properly treat or in some severe cases, quarantine a patient. There have been major development in diagnostic technologies but infectious disease diagnostics are still based on 50-year technologies that are limited by speed of analysis, need for skilled workers, poor detection threshold and inability to detect multiple strains of infectious agents. Here, we describe advances in nanotechnology and microtechnology diagnostics for infectious diseases. In these diagnostic schemes, the nanomaterials are used as labels or barcodes while microfluidic systems are used to automate the sample preparation and the assays. Moreover, we will describe the use of nanotechnology as new approach for treatment of infectious diseases and for vaccine development.
If you want more read
http://www.amazon.com/Nanotechnology-Advances-Medicine-Maysaa-Sayed/dp/1612096409
Friday, September 30, 2011
Nanotechnology and Infectious Disease
Infectious diseases are prevalent in the world and are one of the world's major sources of morbidity and mortality. Though infectious diseases can initiate in a localized region, they can spread rapidly at any moment due to the ease of traveling from one part of the world to the next. This could lead to a global pandemic. One key to preventing this spread is the development of diagnostics technology that can rapidly identify the infectious agent so that one can properly treat or in some severe cases, quarantine a patient. There have been major development in diagnostic technologies but infectious disease diagnostics are still based on 50-year technologies that are limited by speed of analysis, need for skilled workers, poor detection threshold and inability to detect multiple strains of infectious agents. Here, we describe advances in nanotechnology and microtechnology diagnostics for infectious diseases. In these diagnostic schemes, the nanomaterials are used as labels or barcodes while microfluidic systems are used to automate the sample preparation and the assays. Moreover, we will describe the use of nanotechnology as new approach for treatment of infectious diseases and for vaccine development.
If you want more read
http://www.amazon.com/Nanotechnology-Advances-Medicine-Maysaa-Sayed/dp/1612096409
If you want more read
http://www.amazon.com/Nanotechnology-Advances-Medicine-Maysaa-Sayed/dp/1612096409
Thursday, September 29, 2011
Listeria monocytogenes what do you know about?
• Listeria monocytogenes is Gram-positive individually or in short chains
• Non-spore forming
• Motile by means of flagella
• Aerobic
• Optimum growth temperature 30-37°C
• Can grow slowly in refrigerated foods
• There are a 6 different species within the genus but only Listeria monocytogenes is considered pathogenic for humans. Listeria is ubiquitous in the environment. It is quite hardy - resisting freezing, drying and heat. The ability to grow at temperatures as low as 3°C permits multiplication in refrigerated foods.
The organism has served as a model for the study of intracellular pathogenesis for several decades and many aspects of the pathogenic process are well understood
• Listeriae are acquired primarily through the consumption of contaminated foods including soft cheese, raw milk, deli salads, and ready-to-eat foods such as luncheon meats and frankfurters
• Although L. monocytogenes infection is usually limited to individuals that are immunocompromised, the high mortality rate associated with human listeriosis makes L. monocytogenes the leading cause of death amongst foodborne bacterial pathogens .
Approaches for Detection, Identification, and Analysis of Foodborne Pathogens
Traditional microbiological methods for testing foods for the presence of pathogens rely on
Growth in culture media, followed by isolation, and biochemical and serological identification.
Traditional methods are laborious and time consuming, requiring a few days to a week or longer to complete. Rapid detection of pathogens in food is essential for ensuring the safety of food for consumers, and in the past 25 years, advances in biotechnology have resulted in the development of rapid methods that reduce the analysis time.
Major categories of rapid methods include
Immunologic or antibody-based assays
Genetic-based assays such as the polymerase chain reaction.
-Generation assays under development include biosensors and DNA chips that potentially have the capability for near real-time and on-line monitoring for multiple pathogens in foods.
Biosensor-based Detection of Food borne Pathogens
The sensitive, rapid, and specific detection of microorganisms and toxins that taint the food supply has become increasingly important as large-scale manufacture with wide distribution can threaten large populations when a contamination occurs
Listeria has been isolated from products including raw milk, cheese made from unpasteurised milk, soft cheese, ice cream, meat and poultry and fish. Ready to eat meat and poultry products are of particular risk of infection with Listeria.
Listeria monocytogenes bacteria are frequently found in the food-processing environment and can form biofilms on solid surfaces. Listeria is able to survive apparently adverse conditions on smooth surfaces; it thrives in wet, dirty conditions. The presence of Listeria species is a useful hygienic indicator in all stages of the food processing chain. Strains can spread within manufacturing plants and even establish themselves as "house flora".
In susceptible persons an infective dose can be fewer than 100 organisms.
Traditionally food and environmental samples are enriched in a broth prior to subculture into a further broth and then onto selective agar.
The initial broth incubation is at 30°C for 24 hours, the subsequent broth incubation is at 35°C for 24 hours. All broth cultures are then subcultured onto agar for a further 24 hours and subsequently identified by biochemical tests.
The traditional method is labour intensive and takes up to 5 days to give a result. There are therefore now available many commercial alternatives to generate a faster result. One of these is the use of chromogenic agars following a simple 24 hour enrichment. These agars give presumptive positive results.
As an alterative to growth on agar there are a variety of technologies that provide rapid results eg. immunoassay; molecular methods such as PCR; or techniques that reduce time to result e.g. concentration. Sometimes combinations of these techniques are used to further enhance speed to result.
Molecular methods such as PCR can eliminate the need for further identification in the event of a positive and can also provide quantitative information.
The unique challenges of rapid routine environmental monitoring for the presence of Listeria in food processing have been met by specific products.
Following isolation on selective media, identification can be carried out using agglutination, biochemical and molecular techniques.
Latex agglutination allows rapid elimination of negative samples, positives can then be checked out with more targeted tests.
Biochemical profiles identify organisms phenotypically and are widely used.
Molecular methods using PCR or nucleic acid techniques are routinely used as confirmatory tests.
• Non-spore forming
• Motile by means of flagella
• Aerobic
• Optimum growth temperature 30-37°C
• Can grow slowly in refrigerated foods
• There are a 6 different species within the genus but only Listeria monocytogenes is considered pathogenic for humans. Listeria is ubiquitous in the environment. It is quite hardy - resisting freezing, drying and heat. The ability to grow at temperatures as low as 3°C permits multiplication in refrigerated foods.
The organism has served as a model for the study of intracellular pathogenesis for several decades and many aspects of the pathogenic process are well understood
• Listeriae are acquired primarily through the consumption of contaminated foods including soft cheese, raw milk, deli salads, and ready-to-eat foods such as luncheon meats and frankfurters
• Although L. monocytogenes infection is usually limited to individuals that are immunocompromised, the high mortality rate associated with human listeriosis makes L. monocytogenes the leading cause of death amongst foodborne bacterial pathogens .
Approaches for Detection, Identification, and Analysis of Foodborne Pathogens
Traditional microbiological methods for testing foods for the presence of pathogens rely on
Growth in culture media, followed by isolation, and biochemical and serological identification.
Traditional methods are laborious and time consuming, requiring a few days to a week or longer to complete. Rapid detection of pathogens in food is essential for ensuring the safety of food for consumers, and in the past 25 years, advances in biotechnology have resulted in the development of rapid methods that reduce the analysis time.
Major categories of rapid methods include
Immunologic or antibody-based assays
Genetic-based assays such as the polymerase chain reaction.
-Generation assays under development include biosensors and DNA chips that potentially have the capability for near real-time and on-line monitoring for multiple pathogens in foods.
Biosensor-based Detection of Food borne Pathogens
The sensitive, rapid, and specific detection of microorganisms and toxins that taint the food supply has become increasingly important as large-scale manufacture with wide distribution can threaten large populations when a contamination occurs
Listeria has been isolated from products including raw milk, cheese made from unpasteurised milk, soft cheese, ice cream, meat and poultry and fish. Ready to eat meat and poultry products are of particular risk of infection with Listeria.
Listeria monocytogenes bacteria are frequently found in the food-processing environment and can form biofilms on solid surfaces. Listeria is able to survive apparently adverse conditions on smooth surfaces; it thrives in wet, dirty conditions. The presence of Listeria species is a useful hygienic indicator in all stages of the food processing chain. Strains can spread within manufacturing plants and even establish themselves as "house flora".
In susceptible persons an infective dose can be fewer than 100 organisms.
Traditionally food and environmental samples are enriched in a broth prior to subculture into a further broth and then onto selective agar.
The initial broth incubation is at 30°C for 24 hours, the subsequent broth incubation is at 35°C for 24 hours. All broth cultures are then subcultured onto agar for a further 24 hours and subsequently identified by biochemical tests.
The traditional method is labour intensive and takes up to 5 days to give a result. There are therefore now available many commercial alternatives to generate a faster result. One of these is the use of chromogenic agars following a simple 24 hour enrichment. These agars give presumptive positive results.
As an alterative to growth on agar there are a variety of technologies that provide rapid results eg. immunoassay; molecular methods such as PCR; or techniques that reduce time to result e.g. concentration. Sometimes combinations of these techniques are used to further enhance speed to result.
Molecular methods such as PCR can eliminate the need for further identification in the event of a positive and can also provide quantitative information.
The unique challenges of rapid routine environmental monitoring for the presence of Listeria in food processing have been met by specific products.
Following isolation on selective media, identification can be carried out using agglutination, biochemical and molecular techniques.
Latex agglutination allows rapid elimination of negative samples, positives can then be checked out with more targeted tests.
Biochemical profiles identify organisms phenotypically and are widely used.
Molecular methods using PCR or nucleic acid techniques are routinely used as confirmatory tests.
Wednesday, September 28, 2011
Listeria monocytogenes and Food poisoning
Listeria monocytogenes
Listeria monocytogenes is Gram-positive foodborne bacterial pathogen and the causative agent of human listeriosis
The organism has served as a model for the study of intracellular pathogenesis for several decades and many aspects of the pathogenic process are well understood
Listeriae are acquired primarily through the consumption of contaminated foods including soft cheese, raw milk, deli salads, and ready-to-eat foods such as luncheon meats and frankfurters
Although L. monocytogenes infection is usually limited to individuals that are immunocompromised, the high mortality rate associated with human listeriosis makes L. monocytogenes the leading cause of death amongst foodborne bacterial pathogens . As a result, tremendous effort has been made at developing methods for the isolation, detection and control of L. monocytogenes in foods.
Listeria monocytogenes is Gram-positive foodborne bacterial pathogen and the causative agent of human listeriosis
The organism has served as a model for the study of intracellular pathogenesis for several decades and many aspects of the pathogenic process are well understood
Listeriae are acquired primarily through the consumption of contaminated foods including soft cheese, raw milk, deli salads, and ready-to-eat foods such as luncheon meats and frankfurters
Although L. monocytogenes infection is usually limited to individuals that are immunocompromised, the high mortality rate associated with human listeriosis makes L. monocytogenes the leading cause of death amongst foodborne bacterial pathogens . As a result, tremendous effort has been made at developing methods for the isolation, detection and control of L. monocytogenes in foods.
Listeria monocytogenes: What do you know about?
Listeria monocytogenes is a gram-positive facultative anaerobic rod that is a well-known pathogen in the neonate, but it has been increasingly recognized as a pathogen in adults. It can cause infections like meningitis, bacteremia with or without sepsis and chorioamnionitis. Conditions such as advanced age, pregnancy, malignancy, alcoholism, cirrhosis, Crohn's disease, the post-renal transplant state, the treatment with corticosteroids are associated with an increased risk of infection. Listeria monocytogenes is the main pathogenic among the seven known Listeria species [6-9] however rare cases of human disease caused by other species have been reported [6].Techniques for isolation of Listeria monocytogenes included, for all specimens, selective enrichment and cold enrichment that have been shown to increase isolation rates significantly [12]. Subculture was performed after 24 hours on Listeria Selective Medium (Oxford Formulation) has following the methodology and using selective enrichment media described in the literature [13]. Culture was incubated at room temperature for 24-48 hours.
Listeria monocytogenes: What do you know about?
Listeria monocytogenes is a gram-positive facultative anaerobic rod that is a well-known pathogen in the neonate, but it has been increasingly recognized as a pathogen in adults. It can cause infections like meningitis, bacteremia with or without sepsis and chorioamnionitis. Conditions such as advanced age, pregnancy, malignancy, alcoholism, cirrhosis, Crohn's disease, the post-renal transplant state, the treatment with corticosteroids are associated with an increased risk of infection. Listeria monocytogenes is the main pathogenic among the seven known Listeria species [6-9] however rare cases of human disease caused by other species have been reported [6].Techniques for isolation of Listeria monocytogenes included, for all specimens, selective enrichment and cold enrichment that have been shown to increase isolation rates significantly [12]. Subculture was performed after 24 hours on Listeria Selective Medium (Oxford Formulation) has following the methodology and using selective enrichment media described in the literature [13]. Culture was incubated at room temperature for 24-48 hours.
Monday, September 26, 2011
Laboratory associated biological hazards
Historically, workers in diagnostic laboratories have always been at higher risk for infection from exposure to infectious materials. Today, the laboratory worker is faced with increased exposure to infectious material from the recognition of new infectious agents, potential use of bioterrorism agents, increasing antimicrobial resistance, and introduction of new diagnostic techniques and instrumentation. In addition, improper handling of biologic wastes or episodes of laboratory-acquired infection (LAI) could lead to the spread of microorganisms outside the laboratory, although this occurrence has been rare (Harding and Byers, 2000).
LAIs are defined as all infection acquired through laboratory or laboratory-related activities regardless whether they are symptomatic or asymptomatic in nature. LAIs are resulting from occupational exposure to infectious agents (Peterson and Brossette, 2002).
Mode of Transmission and Etiology:
In laboratories, the factors that influence occupationally acquired infections are related to host susceptibility and behavior, the virulence and availability of the pathogen, and the work environment. The most common types of exposure that cause infections include inhalation of aerosols generated by accidents and work practices; percutaneous inoculation through accidents with needles, blades, and broken glassware; ingestion; and contamination of mucous membranes and skin The types of laboratory accidents that are associated with LAIs are listed in Table ( Harding & Byers, 2000).
The manipulation of infectious material in the laboratory often produces aerosol droplets of varying size. Larger droplets rapidly settle from the air and contaminate surfaces. Smaller droplets evaporate and can remain suspended indefinitely. These droplet nuclei (15 urn in diameter) can be inhaled and reach the alveoli of the lungs (Peterson and Brossette, 2002).
Numerous laboratory procedures (e.g., vortexing, mixing, centrifuging, flaming a loop, etc.) produce droplet nuclei. Contact of infectious agents with mucous membranes, conjunctiva, and skin occurs following spills or splashes and accidental aspirations or ingestion. Bench tops, requisitions, equipment, and nearly all items in the laboratory are potentially contaminated (Straton, 2001).
These contaminated items can promote transfer of organisms to mucous membranes through hand-to-face motions or exposure to cuts and abrasions in the skin. Ingestion of infectious materials should not occur through mouth pipetting or food consumption, as these two practices are banned in all clinical laboratories. Laboratory personnel have a high rate of needlesticks and sharp-object accidents that lead to LAIs (Sejvar et al., 2005).
Most of the affected laboratory personnel are microbiologists who may transmit the infection to individuals outside the laboratory. Typhoid fever cases have been associated with handling proficiency test samples and training materials (Straton, 2001).
LAIs are defined as all infection acquired through laboratory or laboratory-related activities regardless whether they are symptomatic or asymptomatic in nature. LAIs are resulting from occupational exposure to infectious agents (Peterson and Brossette, 2002).
Mode of Transmission and Etiology:
In laboratories, the factors that influence occupationally acquired infections are related to host susceptibility and behavior, the virulence and availability of the pathogen, and the work environment. The most common types of exposure that cause infections include inhalation of aerosols generated by accidents and work practices; percutaneous inoculation through accidents with needles, blades, and broken glassware; ingestion; and contamination of mucous membranes and skin The types of laboratory accidents that are associated with LAIs are listed in Table ( Harding & Byers, 2000).
The manipulation of infectious material in the laboratory often produces aerosol droplets of varying size. Larger droplets rapidly settle from the air and contaminate surfaces. Smaller droplets evaporate and can remain suspended indefinitely. These droplet nuclei (15 urn in diameter) can be inhaled and reach the alveoli of the lungs (Peterson and Brossette, 2002).
Numerous laboratory procedures (e.g., vortexing, mixing, centrifuging, flaming a loop, etc.) produce droplet nuclei. Contact of infectious agents with mucous membranes, conjunctiva, and skin occurs following spills or splashes and accidental aspirations or ingestion. Bench tops, requisitions, equipment, and nearly all items in the laboratory are potentially contaminated (Straton, 2001).
These contaminated items can promote transfer of organisms to mucous membranes through hand-to-face motions or exposure to cuts and abrasions in the skin. Ingestion of infectious materials should not occur through mouth pipetting or food consumption, as these two practices are banned in all clinical laboratories. Laboratory personnel have a high rate of needlesticks and sharp-object accidents that lead to LAIs (Sejvar et al., 2005).
Most of the affected laboratory personnel are microbiologists who may transmit the infection to individuals outside the laboratory. Typhoid fever cases have been associated with handling proficiency test samples and training materials (Straton, 2001).
Laboratory associated biological hazards
Historically, workers in diagnostic laboratories have always been at higher risk for infection from exposure to infectious materials. Today, the laboratory worker is faced with increased exposure to infectious material from the recognition of new infectious agents, potential use of bioterrorism agents, increasing antimicrobial resistance, and introduction of new diagnostic techniques and instrumentation. In addition, improper handling of biologic wastes or episodes of laboratory-acquired infection (LAI) could lead to the spread of microorganisms outside the laboratory, although this occurrence has been rare (Harding and Byers, 2000).
LAIs are defined as all infection acquired through laboratory or laboratory-related activities regardless whether they are symptomatic or asymptomatic in nature. LAIs are resulting from occupational exposure to infectious agents (Peterson and Brossette, 2002).
Mode of Transmission and Etiology:
In laboratories, the factors that influence occupationally acquired infections are related to host susceptibility and behavior, the virulence and availability of the pathogen, and the work environment. The most common types of exposure that cause infections include inhalation of aerosols generated by accidents and work practices; percutaneous inoculation through accidents with needles, blades, and broken glassware; ingestion; and contamination of mucous membranes and skin The types of laboratory accidents that are associated with LAIs are listed in Table ( Harding & Byers, 2000).
The manipulation of infectious material in the laboratory often produces aerosol droplets of varying size. Larger droplets rapidly settle from the air and contaminate surfaces. Smaller droplets evaporate and can remain suspended indefinitely. These droplet nuclei (15 urn in diameter) can be inhaled and reach the alveoli of the lungs (Peterson and Brossette, 2002).
Numerous laboratory procedures (e.g., vortexing, mixing, centrifuging, flaming a loop, etc.) produce droplet nuclei. Contact of infectious agents with mucous membranes, conjunctiva, and skin occurs following spills or splashes and accidental aspirations or ingestion. Bench tops, requisitions, equipment, and nearly all items in the laboratory are potentially contaminated (Straton, 2001).
These contaminated items can promote transfer of organisms to mucous membranes through hand-to-face motions or exposure to cuts and abrasions in the skin. Ingestion of infectious materials should not occur through mouth pipetting or food consumption, as these two practices are banned in all clinical laboratories. Laboratory personnel have a high rate of needlesticks and sharp-object accidents that lead to LAIs (Sejvar et al., 2005).
Most of the affected laboratory personnel are microbiologists who may transmit the infection to individuals outside the laboratory. Typhoid fever cases have been associated with handling proficiency test samples and training materials (Straton, 2001).
LAIs are defined as all infection acquired through laboratory or laboratory-related activities regardless whether they are symptomatic or asymptomatic in nature. LAIs are resulting from occupational exposure to infectious agents (Peterson and Brossette, 2002).
Mode of Transmission and Etiology:
In laboratories, the factors that influence occupationally acquired infections are related to host susceptibility and behavior, the virulence and availability of the pathogen, and the work environment. The most common types of exposure that cause infections include inhalation of aerosols generated by accidents and work practices; percutaneous inoculation through accidents with needles, blades, and broken glassware; ingestion; and contamination of mucous membranes and skin The types of laboratory accidents that are associated with LAIs are listed in Table ( Harding & Byers, 2000).
The manipulation of infectious material in the laboratory often produces aerosol droplets of varying size. Larger droplets rapidly settle from the air and contaminate surfaces. Smaller droplets evaporate and can remain suspended indefinitely. These droplet nuclei (15 urn in diameter) can be inhaled and reach the alveoli of the lungs (Peterson and Brossette, 2002).
Numerous laboratory procedures (e.g., vortexing, mixing, centrifuging, flaming a loop, etc.) produce droplet nuclei. Contact of infectious agents with mucous membranes, conjunctiva, and skin occurs following spills or splashes and accidental aspirations or ingestion. Bench tops, requisitions, equipment, and nearly all items in the laboratory are potentially contaminated (Straton, 2001).
These contaminated items can promote transfer of organisms to mucous membranes through hand-to-face motions or exposure to cuts and abrasions in the skin. Ingestion of infectious materials should not occur through mouth pipetting or food consumption, as these two practices are banned in all clinical laboratories. Laboratory personnel have a high rate of needlesticks and sharp-object accidents that lead to LAIs (Sejvar et al., 2005).
Most of the affected laboratory personnel are microbiologists who may transmit the infection to individuals outside the laboratory. Typhoid fever cases have been associated with handling proficiency test samples and training materials (Straton, 2001).
Sunday, September 25, 2011
Peripheral venous catheters
2.2.1 Use the upper extremity for catheter insertion in adults. (1)
2.2.2 Observe the catheter insertion site daily by palpation and
inspection if transparent dressing is used. Visual inspection may
be necessary for opaque dressing if patient has unexplained fever,
pain, local tenderness, other signs of bloodstream infection or
patients cannot communicate. (1, 14)
2.2.3 Replace short, peripheral venous catheter at least every 72-96
hours in adult and remove when no longer indicated. If sites for
venous access are limited, catheter can be maintained for longer
period but close monitoring of insertion site is necessary. Leave
the catheter in place until the therapy is completed, unless a
complication occurs in paediatric patients. (1)2.2.4 Remove the peripheral intravascular catheter if there is sign of
phlebitis or malfunctioning. (1)
2.2.5 Flush the peripheral intravascular lock or needle free device with
normal saline for maintaining the patency and lowering the
overall catheter-related complications though they are not
necessarily infection related. (24)
2.2.6 Efficacy of normal saline solution as an alternative to heparin
solution for the maintenance of peripheral IV devices is to
eliminate the risk of heparin-induced thrombocytopenia,
thrombus, haemorrhage and medication incompatibility which
can provide a safer therapy for patient as well as cost savings. (24,
25, 26). Therefore, normal saline flush is superior and preferable.
2.3 Additional recommendations for peripheral arterial catheters (1)
2.3.1 Use disposable transducer assemblies when possible.
2.3.2 Replace the transducers assemblies at least every 96 hours
together with other components of the system, including the
tubing, continuous-flush device and flush solution.
2.4 Additional recommendations for pressure monitoring system (1)
2.4.1 Keep all components of the system sterile.
2.4.2 Use a closed (continuous) flushing system to maintain the
patency of the system.
2.4.3 Do not infuse the dextrose-containing solution or parenteral
nutrition fluids through the system.
2.5 Umbilical catheters (1)
Avoid tincture of iodine for disinfection of umbilical insertion site in
newborn infants. Other iodine-containing preparation, for example,
povidone iodine, is acceptable.
3 Maintenance of Administration Sets
3.1 Replace administration sets including extension tubings, add-on
devices no more frequently than every 72 hours, unless CABSI is
suspected or confirmed. (1, 27)
3.2 Replace administration sets transfusing blood, blood products or lipid
containing solutions after administration or within 24 hours. (1)3.3 Disinfect IV injection port, stopcocks, needleless intravascular device
or heparin-block with 70% alcohol, 2% Chlorhexidine in alcohol or
iodophor preparation before access. (1, 28, 29)
3.4 IV injection port: there have been reports of higher infection rate
associated with the use of stopcocks (28, 29). When stopcocks are to
be used, cap all stopcocks when not in use. (1)
3.5 Do not draw blood specimens through single-lumen peripheral or
central venous lines intended for infusions except when catheterassociated
bacteremia is suspected. Dedicate a specific lumen from a
multi-lumen for blood-letting. (14)
3.6 Preferably, a single-lumen catheter should be used as it is associated
with reduced risk of CABSI. Multi-lumen catheter should only be
used when there is limited site for iv access.
3.7 Maintain a closed infusion system.
3.7.1 The closed infusion system has been shown to result in
significant reduction in the incidence of CABSI. (30)
3.7.2 The closed infusion system is defined as:
1)the container of intravenous solution is fully collapsible (the
residue after administration does not exceed 5% of the nominal
volume), and hence does not require external air vent to allow the
solution to empty AND
2) the connecting administration set has no air-vent.The whole infusion system is maintained closed to the external
environment while infusing except for the situation listed in para
3.7.3.
3.7.3 In the situation when intravenous solution or medication is
delivered by a semi-rigid plastic or glass bottle, an air vent to
empty the solution is allowed.In-line filters: Do not use filters routinely for infection-control
purposes. (1)
2.2.2 Observe the catheter insertion site daily by palpation and
inspection if transparent dressing is used. Visual inspection may
be necessary for opaque dressing if patient has unexplained fever,
pain, local tenderness, other signs of bloodstream infection or
patients cannot communicate. (1, 14)
2.2.3 Replace short, peripheral venous catheter at least every 72-96
hours in adult and remove when no longer indicated. If sites for
venous access are limited, catheter can be maintained for longer
period but close monitoring of insertion site is necessary. Leave
the catheter in place until the therapy is completed, unless a
complication occurs in paediatric patients. (1)2.2.4 Remove the peripheral intravascular catheter if there is sign of
phlebitis or malfunctioning. (1)
2.2.5 Flush the peripheral intravascular lock or needle free device with
normal saline for maintaining the patency and lowering the
overall catheter-related complications though they are not
necessarily infection related. (24)
2.2.6 Efficacy of normal saline solution as an alternative to heparin
solution for the maintenance of peripheral IV devices is to
eliminate the risk of heparin-induced thrombocytopenia,
thrombus, haemorrhage and medication incompatibility which
can provide a safer therapy for patient as well as cost savings. (24,
25, 26). Therefore, normal saline flush is superior and preferable.
2.3 Additional recommendations for peripheral arterial catheters (1)
2.3.1 Use disposable transducer assemblies when possible.
2.3.2 Replace the transducers assemblies at least every 96 hours
together with other components of the system, including the
tubing, continuous-flush device and flush solution.
2.4 Additional recommendations for pressure monitoring system (1)
2.4.1 Keep all components of the system sterile.
2.4.2 Use a closed (continuous) flushing system to maintain the
patency of the system.
2.4.3 Do not infuse the dextrose-containing solution or parenteral
nutrition fluids through the system.
2.5 Umbilical catheters (1)
Avoid tincture of iodine for disinfection of umbilical insertion site in
newborn infants. Other iodine-containing preparation, for example,
povidone iodine, is acceptable.
3 Maintenance of Administration Sets
3.1 Replace administration sets including extension tubings, add-on
devices no more frequently than every 72 hours, unless CABSI is
suspected or confirmed. (1, 27)
3.2 Replace administration sets transfusing blood, blood products or lipid
containing solutions after administration or within 24 hours. (1)3.3 Disinfect IV injection port, stopcocks, needleless intravascular device
or heparin-block with 70% alcohol, 2% Chlorhexidine in alcohol or
iodophor preparation before access. (1, 28, 29)
3.4 IV injection port: there have been reports of higher infection rate
associated with the use of stopcocks (28, 29). When stopcocks are to
be used, cap all stopcocks when not in use. (1)
3.5 Do not draw blood specimens through single-lumen peripheral or
central venous lines intended for infusions except when catheterassociated
bacteremia is suspected. Dedicate a specific lumen from a
multi-lumen for blood-letting. (14)
3.6 Preferably, a single-lumen catheter should be used as it is associated
with reduced risk of CABSI. Multi-lumen catheter should only be
used when there is limited site for iv access.
3.7 Maintain a closed infusion system.
3.7.1 The closed infusion system has been shown to result in
significant reduction in the incidence of CABSI. (30)
3.7.2 The closed infusion system is defined as:
1)the container of intravenous solution is fully collapsible (the
residue after administration does not exceed 5% of the nominal
volume), and hence does not require external air vent to allow the
solution to empty AND
2) the connecting administration set has no air-vent.The whole infusion system is maintained closed to the external
environment while infusing except for the situation listed in para
3.7.3.
3.7.3 In the situation when intravenous solution or medication is
delivered by a semi-rigid plastic or glass bottle, an air vent to
empty the solution is allowed.In-line filters: Do not use filters routinely for infection-control
purposes. (1)
Recommendations on Prevention of Intravascular Catheter
General Aspects
1.1 Hand hygiene
Perform hand antisepsis with water and antiseptic soap or with alcohol
hand rub for catheter site care and accessing the system, including before
and after catheter insertion, touching the catheter insertion sites, dressing
and the infusion system. (1, 3, 4, 5)
1.2 Use aseptic technique for catheter insertion and catheter site care
1.2.1 Disinfect skin properly before catheter insertion, with sufficient
contact time, (alcohol-based antiseptics require contact time about
30 seconds; non-alcohol-based antiseptics require longer contact
time usually around 2 min) (6). For examples, 70% alcohol for
peripheral line insertion. Chlorhexidine-based preparation is
preferred for central line insertion (1, 7, 8)
1.2.2 Do not use arterial and venous cutdown as a routine method of
catheter insertion. (1)
1.2.3 Use clean gloves and apply “non-touch” technique for peripheral
intravascular catheter insertion after the application of skin
antiseptics. Wear sterile gloves for the insertion of arterial and
central venous catheters. (1)
1.3 Quality assurance, education and surveillance
1.3.1 Implementation of educational programs regarding the indications
for intravascular catheter use, proper procedures for the insertion
and maintenance of intravascular catheters, and appropriate
infection control measures to prevent CABSI. (1, 9, 10)
1.3.2 Ensure persons who insert or manage intravascular catheters are
trained and competent for the procedure.
1.3.3 Well-organized surveillance program that can monitor and
evaluate the performance of care is one of the tools for the
prevention of the CABSI. (1, 9). Both process and outcome
measures on the care of intravascular catheter should be
monitored. For the infection rate, it is preferable to express it by
an incidence density such as “CABSI per 1000 catheter patient
days”. (11)
1.3.4 Do not routinely culture catheter tips unless the source of
infection is likely to be the catheter. (1)
7
1.4 Catheter and site care
1.4.1 Use sterile gauze or transparent dressings to cover the catheter
site. (1). The choice of materials of transparent dressings should
prefer increased durability, improved security of the catheter,
visibility of the wound site, provision of an effective barrier to
micro-organisms or increase the rate of evaporation of fluid. (12,
13)
1.4.2 A gauze dressing is preferred if the site is bleeding, oozing or the
patient is diaphoretic. (1, 14)
1.4.3 Change dressings at least weekly or when clinically indicated
(removal or replacement of catheter; damp, loosened or visibly
soiled dressings). (1)
1.4.4 Secure the catheter after insertion. (1)
1.4.5 Do not apply topical antibiotic ointment or creams to the catheter
insertion site except for dialysis catheters. (1)
1.4.6 Remove the catheter when it is no longer used. (1, 13)
2 Care of Specific Catheters
2.1 Central venous catheters (CVCs), including peripherally inserted
central venous catheters (PICCs), haemodialysis and pulmonary
artery catheters
The central line bundle approach is a group of evidence-based
interventions for patients with intravascular central venous catheters
that, when implemented together, result in better outcomes than when
implemented individually. The central line bundle consists of 5 key
components:
a) Hand hygiene
b) Maximal barrier precautions
c) 2% Chlorhexidine skin antisepsis
d) Optimal catheter site selection, with subclavian vein as the
preferred site for non-tunneled catheters
e) Daily review of line necessity, with prompt removal of unnecessary
lines.
This is not intended to be a comprehensive list of all elements of care
related to central lines. Other elements of care, such as daily site care
and selection of dressing material, are not excluded for any purpose
other than to have a bundle that is focused. (15)
8
2.1.1 A subclavian site is preferred to a jugular or femoral site in adult.
(16, 17, 18, 19) Use a jugular or femoral catheter rather than a
subclavian one for haemodialysis or pheresis. (1)
2.1.2 Use maximal sterile barrier precautions (including the use of cap,
mask, sterile gloves, sterile gown and one large sterile drape) for
insertion of central line. (1, 19, 20)
2.1.3 Minimal numbers of ports and lumens of central venous catheters
essential for management of patients should be used. (1, 21)
2.1.4 Designate a CVC line or one port of a multi-lumen CVC for
exclusive use of parenteral nutrition. (1, 22)
2.1.5 Replace gauze dressing every 2 days and transparent dressing
every 7 days for short-term CVC. The risk of catheter dislodging
should be weighed for changing of dressing in paediatric patients.
(1)
2.1.6 Routine replacement of intravascular catheters is not necessary if
they are functioning and have no evidence of causing local or
systemic complications. (1, 23)
2.1.7 Do not replace intravascular catheters over guidewire if CABSI is
suspected. (1, 23)
2.1.8 Prepare skin with antiseptic chlorhexidine 2% in 70% isopropyl
alcohol which has been proven to provide better skin antisepsis
than other antiseptic agents such as povidine-iodine solutions (1,
15)
1.1 Hand hygiene
Perform hand antisepsis with water and antiseptic soap or with alcohol
hand rub for catheter site care and accessing the system, including before
and after catheter insertion, touching the catheter insertion sites, dressing
and the infusion system. (1, 3, 4, 5)
1.2 Use aseptic technique for catheter insertion and catheter site care
1.2.1 Disinfect skin properly before catheter insertion, with sufficient
contact time, (alcohol-based antiseptics require contact time about
30 seconds; non-alcohol-based antiseptics require longer contact
time usually around 2 min) (6). For examples, 70% alcohol for
peripheral line insertion. Chlorhexidine-based preparation is
preferred for central line insertion (1, 7, 8)
1.2.2 Do not use arterial and venous cutdown as a routine method of
catheter insertion. (1)
1.2.3 Use clean gloves and apply “non-touch” technique for peripheral
intravascular catheter insertion after the application of skin
antiseptics. Wear sterile gloves for the insertion of arterial and
central venous catheters. (1)
1.3 Quality assurance, education and surveillance
1.3.1 Implementation of educational programs regarding the indications
for intravascular catheter use, proper procedures for the insertion
and maintenance of intravascular catheters, and appropriate
infection control measures to prevent CABSI. (1, 9, 10)
1.3.2 Ensure persons who insert or manage intravascular catheters are
trained and competent for the procedure.
1.3.3 Well-organized surveillance program that can monitor and
evaluate the performance of care is one of the tools for the
prevention of the CABSI. (1, 9). Both process and outcome
measures on the care of intravascular catheter should be
monitored. For the infection rate, it is preferable to express it by
an incidence density such as “CABSI per 1000 catheter patient
days”. (11)
1.3.4 Do not routinely culture catheter tips unless the source of
infection is likely to be the catheter. (1)
7
1.4 Catheter and site care
1.4.1 Use sterile gauze or transparent dressings to cover the catheter
site. (1). The choice of materials of transparent dressings should
prefer increased durability, improved security of the catheter,
visibility of the wound site, provision of an effective barrier to
micro-organisms or increase the rate of evaporation of fluid. (12,
13)
1.4.2 A gauze dressing is preferred if the site is bleeding, oozing or the
patient is diaphoretic. (1, 14)
1.4.3 Change dressings at least weekly or when clinically indicated
(removal or replacement of catheter; damp, loosened or visibly
soiled dressings). (1)
1.4.4 Secure the catheter after insertion. (1)
1.4.5 Do not apply topical antibiotic ointment or creams to the catheter
insertion site except for dialysis catheters. (1)
1.4.6 Remove the catheter when it is no longer used. (1, 13)
2 Care of Specific Catheters
2.1 Central venous catheters (CVCs), including peripherally inserted
central venous catheters (PICCs), haemodialysis and pulmonary
artery catheters
The central line bundle approach is a group of evidence-based
interventions for patients with intravascular central venous catheters
that, when implemented together, result in better outcomes than when
implemented individually. The central line bundle consists of 5 key
components:
a) Hand hygiene
b) Maximal barrier precautions
c) 2% Chlorhexidine skin antisepsis
d) Optimal catheter site selection, with subclavian vein as the
preferred site for non-tunneled catheters
e) Daily review of line necessity, with prompt removal of unnecessary
lines.
This is not intended to be a comprehensive list of all elements of care
related to central lines. Other elements of care, such as daily site care
and selection of dressing material, are not excluded for any purpose
other than to have a bundle that is focused. (15)
8
2.1.1 A subclavian site is preferred to a jugular or femoral site in adult.
(16, 17, 18, 19) Use a jugular or femoral catheter rather than a
subclavian one for haemodialysis or pheresis. (1)
2.1.2 Use maximal sterile barrier precautions (including the use of cap,
mask, sterile gloves, sterile gown and one large sterile drape) for
insertion of central line. (1, 19, 20)
2.1.3 Minimal numbers of ports and lumens of central venous catheters
essential for management of patients should be used. (1, 21)
2.1.4 Designate a CVC line or one port of a multi-lumen CVC for
exclusive use of parenteral nutrition. (1, 22)
2.1.5 Replace gauze dressing every 2 days and transparent dressing
every 7 days for short-term CVC. The risk of catheter dislodging
should be weighed for changing of dressing in paediatric patients.
(1)
2.1.6 Routine replacement of intravascular catheters is not necessary if
they are functioning and have no evidence of causing local or
systemic complications. (1, 23)
2.1.7 Do not replace intravascular catheters over guidewire if CABSI is
suspected. (1, 23)
2.1.8 Prepare skin with antiseptic chlorhexidine 2% in 70% isopropyl
alcohol which has been proven to provide better skin antisepsis
than other antiseptic agents such as povidine-iodine solutions (1,
15)
CVC hospital acquired Infections
The Recommendations on Prevention of Intravascular Catheter
Associated Bloodstream Infection (CABSI) represent the second
accomplishment of The Scientific Committee on Infection Control (SCIC) in
the promulgation of preventive measures for the four major systems of
healthcare associated infections namely, surgical site infection, intravascular catheter associated bloodstream infection, ventilator associated pneumonia and catheter associated urinary tract infection. Joining the local parties in the development of the present recommendations, the SCIC has also brought in international renowned expert, Dr Victor D. Rosenthal to provide advice and up-to-date knowledge on closed infusion system during the process. It is believed that the recommendations will provide guidance for the hospital colleagues on good practice in the formulation of strategies, programmes and plans for the prevention of intravascular catheter associated bloodstream infection.
Associated Bloodstream Infection (CABSI) represent the second
accomplishment of The Scientific Committee on Infection Control (SCIC) in
the promulgation of preventive measures for the four major systems of
healthcare associated infections namely, surgical site infection, intravascular catheter associated bloodstream infection, ventilator associated pneumonia and catheter associated urinary tract infection. Joining the local parties in the development of the present recommendations, the SCIC has also brought in international renowned expert, Dr Victor D. Rosenthal to provide advice and up-to-date knowledge on closed infusion system during the process. It is believed that the recommendations will provide guidance for the hospital colleagues on good practice in the formulation of strategies, programmes and plans for the prevention of intravascular catheter associated bloodstream infection.
Friday, September 23, 2011
Mycobacterium tuberculosis Culture
Culture of clinical samples increase the detection of Mycobacterium tuberculosis in patients and are more sensitive than direct microscopic examination. Only 10 to 100 viable organisms are needed to have a positive culture, while a minimum of 5000 to 10.000 acid-fast bacilli per milliliter are required for detection by direct smear.
Thin layer agar (TLA) use a solid medium and is based on the microscopic detection of early mycobacterial growth. This method is able to detect growth within 9–14 days and also allows the initial identification of M. tuberculosis on the basis of its colony morphology. The sample is inoculated on a plate containing Middlebrook 7H11 and Middlebrook 7H11 enriched with PNB (para-nitrobenzoic acid). The detection of growth and its comparison in the two media will help the identification of M. tuberculosis complex since it is expected to grow on 7H11 but not on 7H11+PNB where its growth will be inhibited.
Other recent developments for the rapid detection of mycobacteria include manual methods like the MB-Redox (Heipha Diagnostika Biotest, Heidelberg, Germany) based on the reduction of a tetrazolium salt indicator in liquid medium, and automated equipment-based methods like the MB/BacT system (Organon Teknika, Boxtel, Holland) based on the colorimetric detection of carbon dioxide produced by mycobacterial growth in a closed system, and the ESP culture system II (Trek Diagnostics, Inc., Cleveland, OH, USA) based on the detection of pressure changes in the culture medium of a sealed vial during mycobacterial growth. These systems have not gained widespread use outside laboratories in industrialized countries.
need more read Mycobacterium tuberculosis, current status
Thin layer agar (TLA) use a solid medium and is based on the microscopic detection of early mycobacterial growth. This method is able to detect growth within 9–14 days and also allows the initial identification of M. tuberculosis on the basis of its colony morphology. The sample is inoculated on a plate containing Middlebrook 7H11 and Middlebrook 7H11 enriched with PNB (para-nitrobenzoic acid). The detection of growth and its comparison in the two media will help the identification of M. tuberculosis complex since it is expected to grow on 7H11 but not on 7H11+PNB where its growth will be inhibited.
Other recent developments for the rapid detection of mycobacteria include manual methods like the MB-Redox (Heipha Diagnostika Biotest, Heidelberg, Germany) based on the reduction of a tetrazolium salt indicator in liquid medium, and automated equipment-based methods like the MB/BacT system (Organon Teknika, Boxtel, Holland) based on the colorimetric detection of carbon dioxide produced by mycobacterial growth in a closed system, and the ESP culture system II (Trek Diagnostics, Inc., Cleveland, OH, USA) based on the detection of pressure changes in the culture medium of a sealed vial during mycobacterial growth. These systems have not gained widespread use outside laboratories in industrialized countries.
need more read Mycobacterium tuberculosis, current status

Thursday, September 22, 2011
Samples for Mycobacterium Tuberculosis
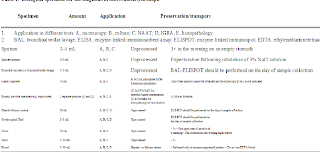
Samples for bacteriological diagnosis usually depends on the affected anatomical sites by infections. The commenest lesion in Mycobacterium tuberculosis is oulmonary infection. Sputum is usually an acceptable sample for diagnosis.
If a patient cannot produce sputum, any method for sputum induction is encouraged. This is especially beneficial to ensure high sensitivity of sputum smear tests in resource-poor settings where such drastic methods as gastric washing or fibro-optic bronchoscopy cannot be used.143 It was shown that induction performed well in developing countries with little added costs.144 Recently, a new device for sputum induction called the ‘lung flute’ has been developed and may be worth trying145 (refer to Table 1 for collecting and processing specimens for the diagnosis of tuberculosis)
If a patient cannot produce sputum, any method for sputum induction is encouraged. This is especially beneficial to ensure high sensitivity of sputum smear tests in resource-poor settings where such drastic methods as gastric washing or fibro-optic bronchoscopy cannot be used.143 It was shown that induction performed well in developing countries with little added costs.144 Recently, a new device for sputum induction called the ‘lung flute’ has been developed and may be worth trying145 (refer to Table 1 for collecting and processing specimens for the diagnosis of tuberculosis)
Wednesday, September 21, 2011
Microbiology Laboratory Quality Control
General Requirements
For moderately and highly complex tests, the laboratory must:
Follow the manufacturer's instructions.
Have a procedure manual describing the process of the tests
and reporting patient test results.
Perform and document calibration procedures or check
calibration at least once every six months.
Perform and document control procedures using at least two levels of controls each day of testing.
Perform and document applicable specialty and subspecialty control procedures.
Perform and document remedial action taken when problems or errors are identified.
Maintain records of all quality control activities for two years (five years for immunohematology).
Facilities
The laboratory must have space and environmental conditions necessary for conducting the services offered. This includes being constructed, arranged and maintained to ensure the space, ventilation and utilities necessary for conducting all phases of testing.
Safety precautions must be established, posted and observed to ensure protection from physical, chemical, biochemical and electrical hazards and biohazardous materials.
Test Methods, Equipment, Instruments, Reagents, Materials and Supplies
The laboratory must utilize test methods, equipment, instruments, reagents, materials and supplies that provide accurate and reliable test results and reports.
Requirements include
-Utilize appropriate and sufficient equipment, instruments, reagents, materials and supplies for the type and volume of testing performed and for the assurance of quality throughout the testing; and, test result reporting, including (as applicable): -Selecting methodologies and equipment and performing testing in a manner that provides test results within the laboratory's stated performance specifications for each method
-Water quality
-Temperature
-Humidity
-Protection of equipment and instrumentation from fluctuations and interruptions in electrical current that adversely affect results and reports
Document remedial actions implemented to correct conditions that fail to meet criteria
-Label reagents, solutions, culture media, control materials, calibration materials and other supplies including identification for:
Storage requirements-
-Identity, and when pertinent, titer, strength or concentration
-Preparation and expiration date Other appropriate information
-Prepare, store and handle reagents, solutions, culture media, control materials, calibration materials and other supplies in a manner to ensure:
- Items are not used when they have exceeded their expiration date, have deteriorated or are of sub-standard quality.
-Components of reagent kits of different lot numbers are not interchanged unless otherwise specified by the manufacturer
Control procedures
Remedial action to be taken when calibration or control results fail to meet the laboratory's criteria for acceptability.
-Limitations in methodologies, including interfering substances
Reference or normal ranges
-Imminent life-threatening laboratory results or panic (critical values. Must be informed at once by telephone to doctor e.g. Meningococci in direct gram of CSF.
-Pertinent literature references
Appropriate criteria for specimen storage and preservation to ensure specimen integrity until testing is completed.
The laboratory's system for reporting patient results including, when appropriate, the protocol for reporting panic values. Description of the steps to be taken in the event that a test system becomes inoperable. Criteria for the referral of specimens including procedures for specimen submission and handling
You can find more in book entiteled Lectures on applied clinical microbiology
For moderately and highly complex tests, the laboratory must:
Follow the manufacturer's instructions.
Have a procedure manual describing the process of the tests
and reporting patient test results.
Perform and document calibration procedures or check
calibration at least once every six months.
Perform and document control procedures using at least two levels of controls each day of testing.
Perform and document applicable specialty and subspecialty control procedures.
Perform and document remedial action taken when problems or errors are identified.
Maintain records of all quality control activities for two years (five years for immunohematology).
Facilities
The laboratory must have space and environmental conditions necessary for conducting the services offered. This includes being constructed, arranged and maintained to ensure the space, ventilation and utilities necessary for conducting all phases of testing.
Safety precautions must be established, posted and observed to ensure protection from physical, chemical, biochemical and electrical hazards and biohazardous materials.
Test Methods, Equipment, Instruments, Reagents, Materials and Supplies
The laboratory must utilize test methods, equipment, instruments, reagents, materials and supplies that provide accurate and reliable test results and reports.
Requirements include
-Utilize appropriate and sufficient equipment, instruments, reagents, materials and supplies for the type and volume of testing performed and for the assurance of quality throughout the testing; and, test result reporting, including (as applicable): -Selecting methodologies and equipment and performing testing in a manner that provides test results within the laboratory's stated performance specifications for each method
-Water quality
-Temperature
-Humidity
-Protection of equipment and instrumentation from fluctuations and interruptions in electrical current that adversely affect results and reports
Document remedial actions implemented to correct conditions that fail to meet criteria
-Label reagents, solutions, culture media, control materials, calibration materials and other supplies including identification for:
Storage requirements-
-Identity, and when pertinent, titer, strength or concentration
-Preparation and expiration date Other appropriate information
-Prepare, store and handle reagents, solutions, culture media, control materials, calibration materials and other supplies in a manner to ensure:
- Items are not used when they have exceeded their expiration date, have deteriorated or are of sub-standard quality.
-Components of reagent kits of different lot numbers are not interchanged unless otherwise specified by the manufacturer
Control procedures
Remedial action to be taken when calibration or control results fail to meet the laboratory's criteria for acceptability.
-Limitations in methodologies, including interfering substances
Reference or normal ranges
-Imminent life-threatening laboratory results or panic (critical values. Must be informed at once by telephone to doctor e.g. Meningococci in direct gram of CSF.
-Pertinent literature references
Appropriate criteria for specimen storage and preservation to ensure specimen integrity until testing is completed.
The laboratory's system for reporting patient results including, when appropriate, the protocol for reporting panic values. Description of the steps to be taken in the event that a test system becomes inoperable. Criteria for the referral of specimens including procedures for specimen submission and handling
You can find more in book entiteled Lectures on applied clinical microbiology
Biosafety Measures in the Clinical Laboratory
Biologic safety cabinets
Clinical laboratories are special, often unique, work environments that may pose identifiable infectious disease risks to persons in or near them. These infections have been recognized for many years. In a series of published early surveys, Pike and associates1-4 reported over 3,000 cases of laboratory-acquired infections, including brucellosis, tuberculosis, typhoid, streptococcal infections, and hepatitis. These incidents, along with considerable anecdotal information, suggest that most laboratory-acquired infections occur as a result of error, accident, or carelessness in the handling of a known pathogen; often the mode of transmission is unknown.
During the 1970s, in an effort to reduce the risks of infection in the laboratory, scientists devised a system for categorizing etiologic agents into groups based on the mode of transmission, type and seriousness of illness resulting from infection, availability of treatment (eg, antimicrobial drugs), and availability of prevention measures (eg, vaccination). The etiologic agent groupings were the basis for the development of guidelines for appropriate facilities, containment equipment, procedures, and work practices to be used by laboratorians. These guidelines, now referred to as biosafety levels 1 through 4, are published and regularly reviewed by the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH).
Biosafety level guidelines recognize that facility design is important in providing a barrier to protect persons working in the facility as well as those in the community. An accidental release of certain airborne infectious agents could be catastrophic. To assist in planning and managing a laboratory, the CDC describes 3 facility designs based on functions in handling infectious agents.
Basic Laboratory
The first design, known as the basic laboratory, provides general space in which work is done with viable biosafety level 1 agents (eg, Bacillus subtilis, Naegleria gruberi), which are not associated with disease in healthy adults, and biosafety level 2 agents (eg, hepatitis B, salmonellae), which pose minimal potential aerosol hazard to laboratory personnel and the environment. Basic laboratories include those that use biosafety levels 1 and 2. While work is commonly conducted on the open bench, certain operations are confined to biologic safety cabinets. Public areas and general offices to which non laboratory staff requires frequent access should be separated from spaces that primarily support laboratory functions.
Biosafety level 2 used in the basic laboratory differs from biosafety level 1 in that:
1. Laboratory personnel have specific training in handling pathogenic agents and are directed by competent scientists;
2. Access to the laboratory is limited when work is being conducted;
3. Extreme precautions are taken with contaminated sharp items; and
4. Certain procedures in which infectious aerosols or splashes may be created are conducted in biologic safety cabinet or other physical containment equipment.
There is no specification for single-pass directional inward flow of air (a system in which air goes through the laboratory area once before being filtered) from a biosafety level 2 laboratory. However, because most microbiology laboratories also work with potentially hazardous chemicals, negative air pressure is usually present as well. There are published recommendations for preventing buildup of chemical vapors in laboratories, including use of chemical fume hoods and/or single-pass air when recirculation would increase the ambient concentration of hazardous materials.
Containment Laboratory
The containment laboratory has special engineering features that make it possible for laboratory personnel to handle aerosolized hazardous materials (eg, Mycobacterium tuberculosis, Coxiella burnetii, and St Louis encephalitis virus) without endangering themselves. More emphasis is placed on primary and secondary barriers to protect personnel in contiguous areas and the community from exposure to potentially infectious aerosols and to prevent contamination of the environment. This laboratory is usually described as a biosafety level 3 facilities.
The unique features that distinguish this laboratory from the basic laboratory are the provisions for access control and a specialized ventilation system. The containment laboratory may be an entire building or a single room (eg, for tuberculosis testing) in a basic laboratory. A containment laboratory is separated from other parts of the building by an anteroom with 2 sets of doors or by access through a basic laboratory area. Because of the potential for aerosol transmission, air movement is unidirectional into the laboratory (ie, from clean areas into the containment area), and all exhaust air is directed outside the building without any recirculation, or it undergoes high-efficiency particulate air (HEPA) filtration.
All procedures involving the manipulation of infectious materials are conducted within biologic safety cabinets or other physical containment devices. These facilities have solid floors and ceilings and sealed penetrations. They are designed and maintained to allow appropriate decontamination in the event of a significant spill. All waste from these laboratories must be rendered noninfectious before final disposal.
Maximum Containment Laboratory
The maximum containment laboratory has special engineering and containment features that allow activities associated with infectious agents (e.g., Lassa virus, Ebola virus) that are extremely hazardous to laboratory personnel or that may cause serious epidemic disease. This laboratory is considered a biosafety level 4 facilities. Although the maximum containment laboratory is usually a separate building, it can be constructed as an isolated area within a building. The laboratory's distinguishing characteristic is that is has secondary barriers to prevent hazardous materials from escaping into the environment. Such barriers include sealed openings into the laboratory, air locks or liquid disinfectant barriers, a clothing-change and shower room contiguous with the laboratory, a double-door autoclave, a biowaste treatment system, a separate ventilation system, and a treatment system to decontaminate exhaust air.
Within work areas of the facility, all activities are confined to class III biologic safety cabinets or class II biologic safety cabinets used by personnel wearing 1-piece positive-pressure body suits ventilated by a life-support system. Members of the laboratory staff have specific and thorough training in handling extremely hazardous infectious agents, and they understand the primary and secondary containment functions of the standard and special practices, the containment equipment, and the laboratory design characteristics. They are supervised by competent scientists who are trained and experienced in working with these agents.
All wastes are decontaminated before leaving the maximum containment laboratory, and the exhaust air is passed through HEPA filters. Except in extraordinary circumstances (eg, suspected hemorrhagic fever), the initial processing of clinical specimens and identification of isolates can be done safely at a lower level containment. The containment elements are consistent with the Occupational Safety and Health Administration Blood borne Pathogen Standard as well as those recommended by the National Committee for Clinical Laboratory Standards (M29-A).
Biologic Safety Cabinets
Various laboratory procedures generate aerosols that may spread biohazardous materials in the work area and pose a risk of infection to personnel. Biologic safety cabinets are used to prevent the escape of aerosols or droplets and to protect the research product from airborne contamination. These devices are distinct from horizontal or vertical laminar flow hoods, which should never be used for handling biohazardous, toxic, or sensitizing material. Chemical fume hoods also should not be used for biohazards as they are solely designed to protect the individual from exposure to chemicals and noxious gases. These chemical fume hoods are not equipped with HEPA filters. BSCs are designed to protect the individual and the environment from biologic agents and to protect the specimens and other materials from biologic contamination.
There are 3 general types of BSCs: class I, II, and III [F1] [F2] and [F3] There is 1 type of class I BSC. This cabinet is similar to a chemical fume hood with an inward airflow through the front opening. The exhaust air from the biologic safety cabinet is passed through a HEPA filter so that the equipment provides protection for the worker and the public. However, the specimens and other materials are potentially subject to contamination. Class I cabinets are not generally recommended for biohazard work.
Class II biologic safety cabinets are designed to protect personnel, the general public, and the specimen. The airflow velocity at the face of the work opening is at least 75 linear feet per minute (lfpm). Both the supply and the exhaust air are HEPA filtered. There are 4 types of class II cabinets (IIA, IIB1, IIB2, and IIB3). They differ in the amount of recirculation, downflow, and inflow. Usually, all but IIA are considered satisfactory for biohazard and toxic agents.
Class III cabinets are totally enclosed, ventilate cabinets of gas-tight construction, and offer the highest degree of protection from infectious aerosols. They also protect research materials from biologic contamination. Class III cabinets are most suitable for work with hazardous agents that require biosafety level 3 or 4 containment. All operations in the work area of the cabinet are performed through attached rubber gloves. The cabinets are operated under negative pressure. Supply air is HEPA filtered, and the cabinet exhaust air is filtered by 2 HEPA filters in series or HEPA filtration followed by incineration, before discharge outside of the facility.
Every day, new organisms are discovered that could potentially become pathogenic to the laboratory staff, patients, and visitors. It is up to the laboratory specialists in infection control, safety, and microbiology to recognize these potential diseases and handle the organisms according to the NIH's most-recent biosafety guidelines.
Clinical laboratories are special, often unique, work environments that may pose identifiable infectious disease risks to persons in or near them. These infections have been recognized for many years. In a series of published early surveys, Pike and associates1-4 reported over 3,000 cases of laboratory-acquired infections, including brucellosis, tuberculosis, typhoid, streptococcal infections, and hepatitis. These incidents, along with considerable anecdotal information, suggest that most laboratory-acquired infections occur as a result of error, accident, or carelessness in the handling of a known pathogen; often the mode of transmission is unknown.
During the 1970s, in an effort to reduce the risks of infection in the laboratory, scientists devised a system for categorizing etiologic agents into groups based on the mode of transmission, type and seriousness of illness resulting from infection, availability of treatment (eg, antimicrobial drugs), and availability of prevention measures (eg, vaccination). The etiologic agent groupings were the basis for the development of guidelines for appropriate facilities, containment equipment, procedures, and work practices to be used by laboratorians. These guidelines, now referred to as biosafety levels 1 through 4, are published and regularly reviewed by the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH).
Biosafety level guidelines recognize that facility design is important in providing a barrier to protect persons working in the facility as well as those in the community. An accidental release of certain airborne infectious agents could be catastrophic. To assist in planning and managing a laboratory, the CDC describes 3 facility designs based on functions in handling infectious agents.
Basic Laboratory
The first design, known as the basic laboratory, provides general space in which work is done with viable biosafety level 1 agents (eg, Bacillus subtilis, Naegleria gruberi), which are not associated with disease in healthy adults, and biosafety level 2 agents (eg, hepatitis B, salmonellae), which pose minimal potential aerosol hazard to laboratory personnel and the environment. Basic laboratories include those that use biosafety levels 1 and 2. While work is commonly conducted on the open bench, certain operations are confined to biologic safety cabinets. Public areas and general offices to which non laboratory staff requires frequent access should be separated from spaces that primarily support laboratory functions.
Biosafety level 2 used in the basic laboratory differs from biosafety level 1 in that:
1. Laboratory personnel have specific training in handling pathogenic agents and are directed by competent scientists;
2. Access to the laboratory is limited when work is being conducted;
3. Extreme precautions are taken with contaminated sharp items; and
4. Certain procedures in which infectious aerosols or splashes may be created are conducted in biologic safety cabinet or other physical containment equipment.
There is no specification for single-pass directional inward flow of air (a system in which air goes through the laboratory area once before being filtered) from a biosafety level 2 laboratory. However, because most microbiology laboratories also work with potentially hazardous chemicals, negative air pressure is usually present as well. There are published recommendations for preventing buildup of chemical vapors in laboratories, including use of chemical fume hoods and/or single-pass air when recirculation would increase the ambient concentration of hazardous materials.
Containment Laboratory
The containment laboratory has special engineering features that make it possible for laboratory personnel to handle aerosolized hazardous materials (eg, Mycobacterium tuberculosis, Coxiella burnetii, and St Louis encephalitis virus) without endangering themselves. More emphasis is placed on primary and secondary barriers to protect personnel in contiguous areas and the community from exposure to potentially infectious aerosols and to prevent contamination of the environment. This laboratory is usually described as a biosafety level 3 facilities.
The unique features that distinguish this laboratory from the basic laboratory are the provisions for access control and a specialized ventilation system. The containment laboratory may be an entire building or a single room (eg, for tuberculosis testing) in a basic laboratory. A containment laboratory is separated from other parts of the building by an anteroom with 2 sets of doors or by access through a basic laboratory area. Because of the potential for aerosol transmission, air movement is unidirectional into the laboratory (ie, from clean areas into the containment area), and all exhaust air is directed outside the building without any recirculation, or it undergoes high-efficiency particulate air (HEPA) filtration.
All procedures involving the manipulation of infectious materials are conducted within biologic safety cabinets or other physical containment devices. These facilities have solid floors and ceilings and sealed penetrations. They are designed and maintained to allow appropriate decontamination in the event of a significant spill. All waste from these laboratories must be rendered noninfectious before final disposal.
Maximum Containment Laboratory
The maximum containment laboratory has special engineering and containment features that allow activities associated with infectious agents (e.g., Lassa virus, Ebola virus) that are extremely hazardous to laboratory personnel or that may cause serious epidemic disease. This laboratory is considered a biosafety level 4 facilities. Although the maximum containment laboratory is usually a separate building, it can be constructed as an isolated area within a building. The laboratory's distinguishing characteristic is that is has secondary barriers to prevent hazardous materials from escaping into the environment. Such barriers include sealed openings into the laboratory, air locks or liquid disinfectant barriers, a clothing-change and shower room contiguous with the laboratory, a double-door autoclave, a biowaste treatment system, a separate ventilation system, and a treatment system to decontaminate exhaust air.
Within work areas of the facility, all activities are confined to class III biologic safety cabinets or class II biologic safety cabinets used by personnel wearing 1-piece positive-pressure body suits ventilated by a life-support system. Members of the laboratory staff have specific and thorough training in handling extremely hazardous infectious agents, and they understand the primary and secondary containment functions of the standard and special practices, the containment equipment, and the laboratory design characteristics. They are supervised by competent scientists who are trained and experienced in working with these agents.
All wastes are decontaminated before leaving the maximum containment laboratory, and the exhaust air is passed through HEPA filters. Except in extraordinary circumstances (eg, suspected hemorrhagic fever), the initial processing of clinical specimens and identification of isolates can be done safely at a lower level containment. The containment elements are consistent with the Occupational Safety and Health Administration Blood borne Pathogen Standard as well as those recommended by the National Committee for Clinical Laboratory Standards (M29-A).
Biologic Safety Cabinets
Various laboratory procedures generate aerosols that may spread biohazardous materials in the work area and pose a risk of infection to personnel. Biologic safety cabinets are used to prevent the escape of aerosols or droplets and to protect the research product from airborne contamination. These devices are distinct from horizontal or vertical laminar flow hoods, which should never be used for handling biohazardous, toxic, or sensitizing material. Chemical fume hoods also should not be used for biohazards as they are solely designed to protect the individual from exposure to chemicals and noxious gases. These chemical fume hoods are not equipped with HEPA filters. BSCs are designed to protect the individual and the environment from biologic agents and to protect the specimens and other materials from biologic contamination.
There are 3 general types of BSCs: class I, II, and III [F1] [F2] and [F3] There is 1 type of class I BSC. This cabinet is similar to a chemical fume hood with an inward airflow through the front opening. The exhaust air from the biologic safety cabinet is passed through a HEPA filter so that the equipment provides protection for the worker and the public. However, the specimens and other materials are potentially subject to contamination. Class I cabinets are not generally recommended for biohazard work.
Class II biologic safety cabinets are designed to protect personnel, the general public, and the specimen. The airflow velocity at the face of the work opening is at least 75 linear feet per minute (lfpm). Both the supply and the exhaust air are HEPA filtered. There are 4 types of class II cabinets (IIA, IIB1, IIB2, and IIB3). They differ in the amount of recirculation, downflow, and inflow. Usually, all but IIA are considered satisfactory for biohazard and toxic agents.
Class III cabinets are totally enclosed, ventilate cabinets of gas-tight construction, and offer the highest degree of protection from infectious aerosols. They also protect research materials from biologic contamination. Class III cabinets are most suitable for work with hazardous agents that require biosafety level 3 or 4 containment. All operations in the work area of the cabinet are performed through attached rubber gloves. The cabinets are operated under negative pressure. Supply air is HEPA filtered, and the cabinet exhaust air is filtered by 2 HEPA filters in series or HEPA filtration followed by incineration, before discharge outside of the facility.
Every day, new organisms are discovered that could potentially become pathogenic to the laboratory staff, patients, and visitors. It is up to the laboratory specialists in infection control, safety, and microbiology to recognize these potential diseases and handle the organisms according to the NIH's most-recent biosafety guidelines.
Tuesday, September 20, 2011
Special prevention for hospital-associated pneumonia
Although prompt use of proper antibiotics is the cornerstone for treating ventilator-associated pneumonia (VAP), there are many non-pharmacological interventions which can significantly reduce risk of VAP incidence. The non-pharmacological interventions are summarized in table
 Recent meta-analysis has also indicated that the following interventions are associated with significantly lower levels of VAP: (i) kinetic bed therapy; (ii) subglottic secretion drainage; (iii) oral decontamination with chlorhexidine; (iv) Proper sterilization of respiratory equipment as shown in table 2
Recent meta-analysis has also indicated that the following interventions are associated with significantly lower levels of VAP: (i) kinetic bed therapy; (ii) subglottic secretion drainage; (iii) oral decontamination with chlorhexidine; (iv) Proper sterilization of respiratory equipment as shown in table 2
 Read more in book entitled
Read more in book entitled
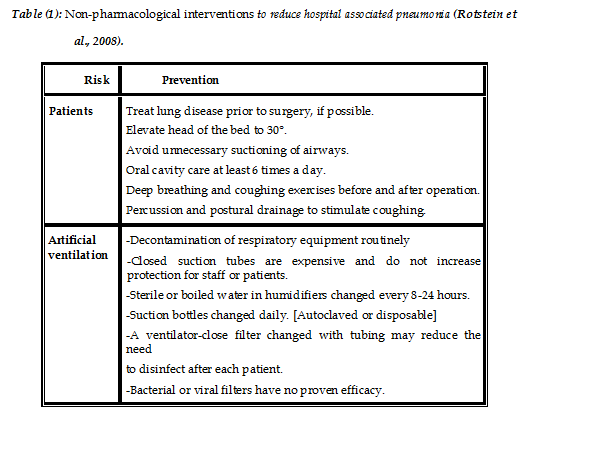

Monday, September 19, 2011
Streptomyces and antibiotics
Streptomyces are Gram-positive, aerobic, high-GC, filamentous soil bacteria known for the production of secondary metabolites and biologically active materials (Stackebrandt et al., 1991).
Streptomycetes are members of the order Actinomycetales within the classes Actinobacteria (Stackebrandt et al., 1997) and have a DNA G+C content of 69±78 mol% (Korn-Wendisch and Kutzner, 1992).
Streptomycetes produce an extensive branching substrate and aerial mycelium. The substrate hyphae are approximately 0.5–2.0 μm in diameter and often lack cross-walls during the vegetative phase. Growth occurs at the hyphal apices and is accompanied by branching, thus producing a complex tightly woven matrix of hyphae during the vegetative growth phase. As the colony ages, aerial mycelia (sporophores) are produced which develop into chains of spores (conidia) by the formation of crosswalls in the multinucleate aerial filaments. This is followed by separation of individual cells directly into spores (Wildermuth and Hopwood, 1970).
The surface of the conidial wall often has convoluted projections which, together with the shape and the arrangement of the spore-bearing structures, are characteristic of each species and were often used for the separation of Streptomyces species (Pridham et al., 1958; Korn-Wendisch and Kutzner, 1992). They can be distinguished from other actinomycetes by their cell wall type which is characterized as Type I sensu (Lechevalier and Lechevalier, 1970b).
Besides antibiotics, which present the largest group of bioactive secondary metabolites, the streptomycete compounds show several other biological activities . The secondary metabolites from streptomycetes can be broadly separated into four classes according to their biological activity: (1) antagonistic agents, including antibacterials, antifungals, antiprotozoans as well as antivirals, (2) pharmacological agents, including antitumorals, immunomodulators, neurological agents and enzyme inhibitors, (3) agrobiologicals, including insecticides, pesticides and herbicides, and (4) compounds with regulatory activities, such as growth factors, siderophores or morphogenic agents. To detect simultaneous bioactivities for a given compound, pharmacological and agricultural screens are increasingly being used in combination with antimicrobial tests. This has revealed several novel therapeutic and agrobiological agents and previously unknown biological activities for antibiotics (Sanglier et al., 1996; Bérdy, 2005). Many reports have shown that since streptomycetes are frequently screened for antimicrobial activity, the existence of secondary metabolites with other activities may have been missed (Garcia et al., 2000; Nunes et al., 2005).
http://www.amazon.com/dp/B005MJAB9O
Streptomycetes are members of the order Actinomycetales within the classes Actinobacteria (Stackebrandt et al., 1997) and have a DNA G+C content of 69±78 mol% (Korn-Wendisch and Kutzner, 1992).
Streptomycetes produce an extensive branching substrate and aerial mycelium. The substrate hyphae are approximately 0.5–2.0 μm in diameter and often lack cross-walls during the vegetative phase. Growth occurs at the hyphal apices and is accompanied by branching, thus producing a complex tightly woven matrix of hyphae during the vegetative growth phase. As the colony ages, aerial mycelia (sporophores) are produced which develop into chains of spores (conidia) by the formation of crosswalls in the multinucleate aerial filaments. This is followed by separation of individual cells directly into spores (Wildermuth and Hopwood, 1970).
The surface of the conidial wall often has convoluted projections which, together with the shape and the arrangement of the spore-bearing structures, are characteristic of each species and were often used for the separation of Streptomyces species (Pridham et al., 1958; Korn-Wendisch and Kutzner, 1992). They can be distinguished from other actinomycetes by their cell wall type which is characterized as Type I sensu (Lechevalier and Lechevalier, 1970b).
Besides antibiotics, which present the largest group of bioactive secondary metabolites, the streptomycete compounds show several other biological activities . The secondary metabolites from streptomycetes can be broadly separated into four classes according to their biological activity: (1) antagonistic agents, including antibacterials, antifungals, antiprotozoans as well as antivirals, (2) pharmacological agents, including antitumorals, immunomodulators, neurological agents and enzyme inhibitors, (3) agrobiologicals, including insecticides, pesticides and herbicides, and (4) compounds with regulatory activities, such as growth factors, siderophores or morphogenic agents. To detect simultaneous bioactivities for a given compound, pharmacological and agricultural screens are increasingly being used in combination with antimicrobial tests. This has revealed several novel therapeutic and agrobiological agents and previously unknown biological activities for antibiotics (Sanglier et al., 1996; Bérdy, 2005). Many reports have shown that since streptomycetes are frequently screened for antimicrobial activity, the existence of secondary metabolites with other activities may have been missed (Garcia et al., 2000; Nunes et al., 2005).
http://www.amazon.com/dp/B005MJAB9O
Sunday, September 18, 2011
What is Actinomycetes ?
Actinomycetes were originally considered to be an intermediate group between bacteria and fungi but are now recognized as prokaryotic. The gram-positive bacteria include two major branches: the low G+C organisms, containing genera such as Bacillus, Closdridium, Staphylococcus and Streptococcus; and the high G+C (> 55%) organisms referred to as the actinomycetes. The majority of the actinomycetes are free living, saprophytic bacteria found widely distributed in soil, water and colonizing plants. Actinomycetes population has been identified as one of the major group of soil population, which may vary with the soil type (Küster, 1968).
Actinomycetes belong to the order Actinomycetales (Superkingdom: Bacteria, Phylum: Firmicutes, Class: Actinobacteria, Subclass: Actinobacteridae). According to Bergey's Manual actinomycetes are divided into eight diverse families: Actinomycetaceae, Mycobacteriaceae, Actinoplanaceae, Frankiaceae, Dermatophilaceae, Nocardiaceae, Streptomycetaceae, Micromonosporaceae (Holt, 1989) and comprise 63 genera (Nisbet and Fox, 1991).
All members of the Streptomycetaceae family have a complex life cycle. They contain specific menaquinones, incorporate LL-diaminopimelic acid (a diagnostic amino acid) into their peptidoglycan, but lack a diagnostic sugar (Schrempf, 2006). An enormous number (>800) of Streptomyces species has been described by numerical taxonomy (Goodfellow et al., 1990). Streptomyces are aerobic, filamentous soil bacteria known for the production of secondary metabolites and biologically active materials (Stackebrandt et al., 1991).
Among microorganisms, actinomycetes are one of the most attractive sources of all types of bioactive metabolites that have important applications in human medicine (Watve et al., 2001). Streptomycetes and related actinomycetes continue to be useful sources of novel secondary metabolites with a range of biological activities that may ultimately find application as anti-infectives, anti-cancer agents or other pharmaceutically useful compounds (Bibb, 2005). Members of Streptomyces are a rich source of bioactive compounds, notably antibiotics, enzymes, enzyme inhibitors and pharmacologically active agents (Yamanaka et al., 2005; Sanglier et al., 1993). About 75 % of the known commercially and medically useful antibiotics are produced by Streptomyces (Sujatha et al., 2005; Takano, 2006).
Antibiotics are antimicrobial compounds produced by living microorganisms. These compounds were used therapeutically and some times prophylactically in the control of infectious diseases. Many antibiotics were produced by microorganisms as secondary metabolites (Ahmed, 2007). Most of the known antibiotics were isolated from some species belonging to actinomycetes and many of them were isolated from genus Streptomyces (Waskman, 1959a) for example 4-methylaeruginoic was isolated from Streptomyces sp. (Henriksen et al., 1998).
The screening programs for new Streptomyces and for their antibiotics are still proceeding at a very rapid pace. There is a need for the development of new antibiotics to overcome the problems associated with toxicity of some used antibiotics and the increase of resistant pathogenic bacteria. To discover the new antibiotics it will be necessary to continue the use of conventional screening programs. Different soils all over the world had been exploited in search of bioactive Streptomyces (Abdelghani et al., 2009; Laidi et al., 2008).
Actinomycetes belong to the order Actinomycetales (Superkingdom: Bacteria, Phylum: Firmicutes, Class: Actinobacteria, Subclass: Actinobacteridae). According to Bergey's Manual actinomycetes are divided into eight diverse families: Actinomycetaceae, Mycobacteriaceae, Actinoplanaceae, Frankiaceae, Dermatophilaceae, Nocardiaceae, Streptomycetaceae, Micromonosporaceae (Holt, 1989) and comprise 63 genera (Nisbet and Fox, 1991).
All members of the Streptomycetaceae family have a complex life cycle. They contain specific menaquinones, incorporate LL-diaminopimelic acid (a diagnostic amino acid) into their peptidoglycan, but lack a diagnostic sugar (Schrempf, 2006). An enormous number (>800) of Streptomyces species has been described by numerical taxonomy (Goodfellow et al., 1990). Streptomyces are aerobic, filamentous soil bacteria known for the production of secondary metabolites and biologically active materials (Stackebrandt et al., 1991).
Among microorganisms, actinomycetes are one of the most attractive sources of all types of bioactive metabolites that have important applications in human medicine (Watve et al., 2001). Streptomycetes and related actinomycetes continue to be useful sources of novel secondary metabolites with a range of biological activities that may ultimately find application as anti-infectives, anti-cancer agents or other pharmaceutically useful compounds (Bibb, 2005). Members of Streptomyces are a rich source of bioactive compounds, notably antibiotics, enzymes, enzyme inhibitors and pharmacologically active agents (Yamanaka et al., 2005; Sanglier et al., 1993). About 75 % of the known commercially and medically useful antibiotics are produced by Streptomyces (Sujatha et al., 2005; Takano, 2006).
Antibiotics are antimicrobial compounds produced by living microorganisms. These compounds were used therapeutically and some times prophylactically in the control of infectious diseases. Many antibiotics were produced by microorganisms as secondary metabolites (Ahmed, 2007). Most of the known antibiotics were isolated from some species belonging to actinomycetes and many of them were isolated from genus Streptomyces (Waskman, 1959a) for example 4-methylaeruginoic was isolated from Streptomyces sp. (Henriksen et al., 1998).
The screening programs for new Streptomyces and for their antibiotics are still proceeding at a very rapid pace. There is a need for the development of new antibiotics to overcome the problems associated with toxicity of some used antibiotics and the increase of resistant pathogenic bacteria. To discover the new antibiotics it will be necessary to continue the use of conventional screening programs. Different soils all over the world had been exploited in search of bioactive Streptomyces (Abdelghani et al., 2009; Laidi et al., 2008).
Saturday, September 17, 2011
Important health care acquired infections in chest hospitals
1. Air borne infections
Close proximity of persons together with handling of human secretions (e.g.: respiratory secretions) make health care workers particularly vulnerable to transmission of droplet-transmitted respiratory infections. This was tragically highlighted during the international outbreak of severe acute respiratory syndrome (SARS) in 2003 with attack rates of more than 50% in health care workers (HCW) before infection control measures were instituted (Pieris et al, 2003)
a. Hospital acquired Tuberculosis
Tuberculosis (TB) is one of the major death-threatening contagious diseases in the world. Although TB is curable, it kills 5000 people every day (World Health Organization, 2006a).
Transmission of M. tuberculosis is a recognized risk to patients and health-care workers (HCWs) in health-care facilities. Transmission is most likely to occur from patients who have unrecognized pulmonary or laryngeal TB, are not on effective anti-tuberculosis therapy, and have not been placed in isolation (Sharon et al., 2009).
Several recent TB outbreaks in health-care facilities, including outbreaks of multidrug-resistant TB (MDR-TB), have heightened concern about nosocomial transmission. Patients who have MDR-TB can remain infectious for prolonged periods, which increase the risk for transmission (Kilinc et al., 2002).
Examples of such healthcare acquired transmission of TB have been reported both locally and internationally. During the late 1980's and early 1990's in the United States, for instance, a healthcare acquired cluster of TB transmission occurred which affected both patients and healthcare workers. Between 2002 and 2003 in Taiwan, there were 19 suspected clusters of healthcare acquired TB infection that occurred in hospitals and nursing institutions (Kilinc et al., 2002).
The healthcare acquired TB clusters mainly resulted from inadequate implementation of infection control measures, delay in diagnosing and confirming TB cases, lack of healthy practices, healthcare workers' poor immunity due to mandatory periodic night shifts and subsequent work fatigue. Also, careless contacts among nursing staff might be one of the reasons that contributed to the nosocomial infection (Margarita et al., 2006).
b. Health care-associated pneumonia HCAP
HAP is defined as pneumonia that occurs 48 hours or more after admission, and that was not incubating at the time of admission. VAP refers to pneumonia that occurs more than 48 hours after endotracheal intubation. HCAP includes the following patients with pneumonia: hospitalized in an acute care hospital for more than 2 days within 90 days of the pneumonia; resided in a long-term care facility (e.g., nursing home); received recent parenteral antimicrobial therapy, chemotherapy, or wound care within 30 days of pneumonia; or received treatment in a hospital or hemodialysis clinic. For practical purposes, most principles for HCAP, VAP, and HAP will overlap. (Chinsky, 2002).
Hospital-acquired pneumonia (HAP) is considered the second most-frequent cause of healthcare acquired infection, accounting for 15 to 20% of these infections. It usually occurs in patients with underlying diseases associated with significant morbidity and mortality and increased costs of treatment. HAP is associated with crude mortality rates of up to 70% and attributable mortality rates as high as 33% to 50%. Many of these deaths may be caused by ventilator-associated pneumonia (VAP), which is believed to be the most frequent infection in patients admitted to the intensive care unit (ICU) (Marcos et al. 2004).
You need to read more: Read at
http://www.amazon.com/dp/B005MJAB9O
Close proximity of persons together with handling of human secretions (e.g.: respiratory secretions) make health care workers particularly vulnerable to transmission of droplet-transmitted respiratory infections. This was tragically highlighted during the international outbreak of severe acute respiratory syndrome (SARS) in 2003 with attack rates of more than 50% in health care workers (HCW) before infection control measures were instituted (Pieris et al, 2003)
a. Hospital acquired Tuberculosis
Tuberculosis (TB) is one of the major death-threatening contagious diseases in the world. Although TB is curable, it kills 5000 people every day (World Health Organization, 2006a).
Transmission of M. tuberculosis is a recognized risk to patients and health-care workers (HCWs) in health-care facilities. Transmission is most likely to occur from patients who have unrecognized pulmonary or laryngeal TB, are not on effective anti-tuberculosis therapy, and have not been placed in isolation (Sharon et al., 2009).
Several recent TB outbreaks in health-care facilities, including outbreaks of multidrug-resistant TB (MDR-TB), have heightened concern about nosocomial transmission. Patients who have MDR-TB can remain infectious for prolonged periods, which increase the risk for transmission (Kilinc et al., 2002).
Examples of such healthcare acquired transmission of TB have been reported both locally and internationally. During the late 1980's and early 1990's in the United States, for instance, a healthcare acquired cluster of TB transmission occurred which affected both patients and healthcare workers. Between 2002 and 2003 in Taiwan, there were 19 suspected clusters of healthcare acquired TB infection that occurred in hospitals and nursing institutions (Kilinc et al., 2002).
The healthcare acquired TB clusters mainly resulted from inadequate implementation of infection control measures, delay in diagnosing and confirming TB cases, lack of healthy practices, healthcare workers' poor immunity due to mandatory periodic night shifts and subsequent work fatigue. Also, careless contacts among nursing staff might be one of the reasons that contributed to the nosocomial infection (Margarita et al., 2006).
b. Health care-associated pneumonia HCAP
HAP is defined as pneumonia that occurs 48 hours or more after admission, and that was not incubating at the time of admission. VAP refers to pneumonia that occurs more than 48 hours after endotracheal intubation. HCAP includes the following patients with pneumonia: hospitalized in an acute care hospital for more than 2 days within 90 days of the pneumonia; resided in a long-term care facility (e.g., nursing home); received recent parenteral antimicrobial therapy, chemotherapy, or wound care within 30 days of pneumonia; or received treatment in a hospital or hemodialysis clinic. For practical purposes, most principles for HCAP, VAP, and HAP will overlap. (Chinsky, 2002).
Hospital-acquired pneumonia (HAP) is considered the second most-frequent cause of healthcare acquired infection, accounting for 15 to 20% of these infections. It usually occurs in patients with underlying diseases associated with significant morbidity and mortality and increased costs of treatment. HAP is associated with crude mortality rates of up to 70% and attributable mortality rates as high as 33% to 50%. Many of these deaths may be caused by ventilator-associated pneumonia (VAP), which is believed to be the most frequent infection in patients admitted to the intensive care unit (ICU) (Marcos et al. 2004).
You need to read more: Read at
http://www.amazon.com/dp/B005MJAB9O
Antibiotics Resistence and Hospital Acquired Infections
Infections have been the major cause of disease throughout the history of human population. With the introduction of antibiotics, it was thought that this problem should disappear. However, bacteria have been able to resist the action of antibiotics. Resistance to antibiotics is a major obstacle in the treatment of infectious diseases, leading to treatment failure and increased treatments' costs.
Bacterial resistance to antibiotics is subdivided into two categories, innate and acquired. Innate resistance is attributed to physiological factors inherently present in the bacteria rendering it immune to certain antibiotics.
Acquired resistance is driven by two genetic processes in bacteria:
• Mutation and selection (sometimes referred to as vertical evolution);
• Exchange of genes between strains and species (sometimes called horizontal evolution). Some bacterial species are able to spread drug resistance to other strains and species during genetic exchange processes.
A number of resistance genes have been associated with large plasmids, on which many other mobile elements; as transposons and integrons are present.
These DNA mobile elements have been shown to possess genetic determinants for several different antibiotic resistance mechanisms and are largely responsible for the rapid dissemination of resistance genes among different bacterial genera and species.
Bacterial resistance to antibiotics is manifested by changes in antibiotic permeability, alteration of target molecules, enzymatic degradation of the antibiotics, and efflux of antimicrobials from the cytoplasm. Bacteria use all of these mechanisms to evade the toxic effects of antibiotics.
HAIs are the most frequent and widely studied adverse effect of hospitalization. They have emerged as an important public health problem and are a leading cause of morbidity and mortality in both developed and developing countries. HAIs results in unnecessary human suffering and death as well as health care expenditures.
The burden of HAIs increased during the past decade due to the increase in immuno-comprimised patients in hospitals, the development of more delicate life support treatments, advanced surgical operations, increasing numbers of elderly patients, more complex hospital environments, and failures in infection control measures.
They can affect any part of the body, but respiratory tract infections, central line infections, urinary tract infections, and wound infections are the most common sites.
In addition to their association with increased morbidity and mortality, HAIs are frequently caused by drug resistant micro-organisms, including MRSA, VRE, and ESBL-producing gram negative bacteria, which pose considerable therapeutic problems.
The main cause of this problem is multifactorial, including selective pressure that results from inappropriate use of antibiotics, Poor hand hygiene by hospital staff and poor quality infection control in the belief that infection has been beaten by antibiotics.
The number of antibiotics belonging to various families, their various modes of action and the number of bacteria in which antibiotic resistance has been documented suggest that, in principle, any microbe could develop resistance to any antibiotic.
Antibiotic resistance is found among essentially all the major bacterial pathogens, and the emergence of multi-resistant ‘super bugs’ within hospitals now poses a very real and formidable threat.
Determining the antimicrobial susceptibility profile of a pathogen is considered as important as the identification of the pathogen involved in the infection. This is becoming more essential in an era of increasing antimicrobial resistance, in which treatment options are limited to newer, more costly antimicrobial agents.
Susceptibility testing in most clinical microbiology laboratories represents a combination of phenotypic assays and molecular-based tests. Phenotypic assays provide either qualitative results (susceptible, intermediate, or resistant) for a series of antimicrobial agents, or quantitative results (MICs) that can guide dosing regimens. Molecular-based tests, such as real-time PCR, may provide rapid information on the presence of MRSA or VRE in patients, which will assist in infection control decisions.
Hospital infection control programs are seen as very important for the control of antibiotic-resistant organisms. Other considerations for an infection control program include antibiotic control programs and surveillance systems for infections with nosocomial pathogens. This type of surveillance is essential for establishing endemic rates.
http://www.amazon.com/Manual-Antibiotics-Mechanisms-Resistance-ebook/dp/B0050VQWXI
Bacterial resistance to antibiotics is subdivided into two categories, innate and acquired. Innate resistance is attributed to physiological factors inherently present in the bacteria rendering it immune to certain antibiotics.
Acquired resistance is driven by two genetic processes in bacteria:
• Mutation and selection (sometimes referred to as vertical evolution);
• Exchange of genes between strains and species (sometimes called horizontal evolution). Some bacterial species are able to spread drug resistance to other strains and species during genetic exchange processes.
A number of resistance genes have been associated with large plasmids, on which many other mobile elements; as transposons and integrons are present.
These DNA mobile elements have been shown to possess genetic determinants for several different antibiotic resistance mechanisms and are largely responsible for the rapid dissemination of resistance genes among different bacterial genera and species.
Bacterial resistance to antibiotics is manifested by changes in antibiotic permeability, alteration of target molecules, enzymatic degradation of the antibiotics, and efflux of antimicrobials from the cytoplasm. Bacteria use all of these mechanisms to evade the toxic effects of antibiotics.
HAIs are the most frequent and widely studied adverse effect of hospitalization. They have emerged as an important public health problem and are a leading cause of morbidity and mortality in both developed and developing countries. HAIs results in unnecessary human suffering and death as well as health care expenditures.
The burden of HAIs increased during the past decade due to the increase in immuno-comprimised patients in hospitals, the development of more delicate life support treatments, advanced surgical operations, increasing numbers of elderly patients, more complex hospital environments, and failures in infection control measures.
They can affect any part of the body, but respiratory tract infections, central line infections, urinary tract infections, and wound infections are the most common sites.
In addition to their association with increased morbidity and mortality, HAIs are frequently caused by drug resistant micro-organisms, including MRSA, VRE, and ESBL-producing gram negative bacteria, which pose considerable therapeutic problems.
The main cause of this problem is multifactorial, including selective pressure that results from inappropriate use of antibiotics, Poor hand hygiene by hospital staff and poor quality infection control in the belief that infection has been beaten by antibiotics.
The number of antibiotics belonging to various families, their various modes of action and the number of bacteria in which antibiotic resistance has been documented suggest that, in principle, any microbe could develop resistance to any antibiotic.
Antibiotic resistance is found among essentially all the major bacterial pathogens, and the emergence of multi-resistant ‘super bugs’ within hospitals now poses a very real and formidable threat.
Determining the antimicrobial susceptibility profile of a pathogen is considered as important as the identification of the pathogen involved in the infection. This is becoming more essential in an era of increasing antimicrobial resistance, in which treatment options are limited to newer, more costly antimicrobial agents.
Susceptibility testing in most clinical microbiology laboratories represents a combination of phenotypic assays and molecular-based tests. Phenotypic assays provide either qualitative results (susceptible, intermediate, or resistant) for a series of antimicrobial agents, or quantitative results (MICs) that can guide dosing regimens. Molecular-based tests, such as real-time PCR, may provide rapid information on the presence of MRSA or VRE in patients, which will assist in infection control decisions.
Hospital infection control programs are seen as very important for the control of antibiotic-resistant organisms. Other considerations for an infection control program include antibiotic control programs and surveillance systems for infections with nosocomial pathogens. This type of surveillance is essential for establishing endemic rates.
http://www.amazon.com/Manual-Antibiotics-Mechanisms-Resistance-ebook/dp/B0050VQWXI
Acquired Antibiotic Resistance
It results from altered cellular physiology and structure caused by changes in a microorganism's genetic makeup. It is unpredictable character and results from mutations or other mechanisms of genetic exchange (Reddy, 2009b).
Through the study of bacterial structure, antibiotics can be designed specifically to overcome the natural barrier of intrinsic resistance in order to successfully target specific organisms. However, much of the antimicrobial resistance associated with nosocomial infections falls into the category of acquired resistance (Spratt and Wade, 2005).
Through the study of bacterial structure, antibiotics can be designed specifically to overcome the natural barrier of intrinsic resistance in order to successfully target specific organisms. However, much of the antimicrobial resistance associated with nosocomial infections falls into the category of acquired resistance (Spratt and Wade, 2005).
Wednesday, September 14, 2011
Mechanisms of Antibiotic Action
Antimicrobial substance is any substance of natural, semisynthetic, or synthetic origin that at in vivo concentrations kills or inhibits the growth of micro-organisms by interacting with a specific target (Cerf et al., 2010).

While antibiotics are natural antimicrobial agents produced by microorganisms such as fungi, actinomycetes and bacteria that is capable in small concentrations to kill or inhibit the growth of other bacteria. However, in common usage antibiotic means antibacterial agent, excluding agents with antiviral and antifungal activity (Bauman, 2009b).
It is hard to imagine hospital medicine in the preantibiotic era, indeed many of the great advances of modern medicine and surgery would not have been possible without the ability to rely on antibiotics to cure secondary infections (Mackenzie et al., 2007).
Mechanisms of antibiotic action:
Antibiotics target structures and pathways that are unique and important to bacteria such as cell wall synthesis, cytoplasmic membrane synthesis, protein synthesis, nucleic acid (DNA or RNA) synthesis and intermediary metabolism (McCallum, 2010).
A-Inhibition of cell wall synthesis:
Bacterial cell wall function and structure:
A cell wall maintains cellular integrity by countering the effects of osmosis when the cell is in a hypotonic solution. If the wall is disrupted, it no longer prevents the cell from bursting as water moves into the cell by osmosis (Dmitriev et al., 2005).
The major structural component of a bacterial cell wall is its peptidoglycan layer. Peptidoglycan is a huge macromolecule composed of polysaccharide chains of alternating N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) molecules that are cross linked by short peptide chains extending between NAM subunits. To enlarge or divide, a cell must synthesize more peptidoglycan by adding new NAG and NAM subunits to existing NAG-NAM chains, and the new NAM subunits must then be bonded to neighboring NAM subunits (Meroueh et al., 2006).
B-Inhibition of cytoplasmic membrane:
Beneath the cell wall, the cytoplasmic membrane essentially acts as a bag that contains the cytoplasm and controls the passage of chemicals into and out of the cell. Extensive damage to membranes' proteins or phospholipids allows the cellular contents to leak out and if not immediately repaired causes death (Manuselis and Mahon, 2007).
Polymyxin B, polymyxin E (colistin), amphotricin B, imidazoles, triazoles and polyenes exert their actions by altering the bacterial cell membranes. The inhibition of cell membrane function leads to escape of macromolecules from the cell resulting in cell damage or death (Chakraborty, 2009).
Polymyxin is effective against gram-negative bateria, particularly pseudomonas, but because it is toxic to human kidneys it is usually reserved for use against pathogens that are resistant to other antibacterial drugs (Bauman, 2009b).
Daptomycin is a new lipopeptide antibiotic that is rapidly bactericidal by binding to the cell membrane in a calcium dependent manner causing depolarization of bacterial membrane potential. This leads to intracellular potassium release. This agent has been approved for use in the treatment of Staphylococcus aureus blood stream infections and skin and soft tissue infections caused by gram-positive bacteria, particularly those organisms that are highly resistant to β-lactam agents and vancomycin (Brooks and Carroll, 2010).
C-Inhibition of protein synthesis:
Cells use proteins for structure and regulation, as enzymes in metabolism and as channels and pumps to move materials across cell membranes. Thus, a consistent supply of proteins is vital for the active life of a cell (Bauman, 2009a).
Many antimicrobial agents take the advantage of the differences between prokaryotic ribosomes (70S) and the eukaryotic ribosomes (80S) to selectively target bacterial protein translation without significantly affecting eukaryotes (Franceschi and Duffy, 2006).
The 70S ribosome is composed of two subunits 30S and 50S built with RNA and proteins (30S composed of 16S rRNA and ribosomal proteins, 50S subunit composed of 23S rRNA, 5S rRNA and ribosomal proteins) which assemble to produce a functional structure for protein synthesis. Each part undertakes a specific function. The small subunit 30S decodes mRNA. In the large 50S part, the protein is formed by the polymerization of amino acids according to the genetic code. tRNA molecules carry the amino acids. Ribosomes possess three tRNA binding sites A, P, and E, hosting the aminoacyl-tRNA, the peptidyl-tRNA, and the exiting tRNA, respectively. Each elongation cycle involves the advancement of the mRNA together with A→ P → E site passage of the tRNA molecule (Agmon et al., 2004).
Antibiotics that target the 30S ribosomal subunit:
• Aminoglycosides:
The aminoglycosides antibiotics (streptomycin, gentamycin, tobramycin, spectinomycin, kanamycin, neomycin and paromycin) are closely related drugs. They have action against a wide range of micro-organisms (Chakraborty, 2009).
The mode of action of streptomycin has been studied more intensively than other aminoglycosides, but all probably act similarly. The first step is the attachment of the aminoglycoside to a specific receptor protein (S12 in the case of streptomycin) on the 30S subunit of the microbial ribosome. Second, the aminoglycoside blocks the normal activity of the "initiation complex" of peptide formation (mRNA + formyl methionine + tRNA). Third, the mRNA message is misread on the "recognition region" of the ribosome; consequently, the wrong amino acid is inserted into the peptide, resulting in a non functional protein. Fourth, aminoglycoside attachment results in break up of polysomes and their separation into monosomes incapable of protein synthesis (Brooks and Carroll, 2010).
• Tetracyclines:
Tetracyclins bind to the 30S ribosomal subunit and inhibit protein synthesis by blocking the attachment of incoming aminoacyl-tRNA. Thus they prevent introduction of new amino acids to the growing peptide chain (Chopra and Roberts, 2001).
Antibiotics that target the 50S ribosomal subunit:
• Chloramphenicol:
The molecular target for chloramphenicol is the peptidyl transferase enzyme that links amino acids in the growing peptide chain. The effect of the antibiotic is thus to freeze the process of chain elongation, bringing bacterial growth to an abrupt halt. The process is completely reversible, and chloramphenicol is fundamentally a bacteriostatic agent (Biswas et al., 2008).
• Macrolides, Lincosamide and streptogramins :
Macrolides, lincosamides, and streptogramin B (MLSB) antibiotics are structurally dissimilar, but are grouped together due to a common mechanism of action. Macrolides include the drugs erythromycin, clarithromycin, and azithromycin. Clindamycin is the main lincosamide used clinically. Quinupristin, combined with streptogramin A dalfopristin, is the most commonly used streptogramin B antibiotic (Champney and Tober, 2000).
The binding site of these drugs is the 23S of bacterial ribosomal RNA. Binding of the antibiotic prevents movement of the ribosome from one codon to the next; as a result, translation is frozen and protein synthesis is halted (Tsui et al., 2004).
• Oxazolidinones:
The oxazolidinones are a relatively new class of antibiotics. These antibiotics inhibit bacterial growth by interfering with the 50S particle assembly and the binding of aminoacyl-tRNA to the ribosomal A site, as shown for linezolid (Leach et al., 2007).
read more at
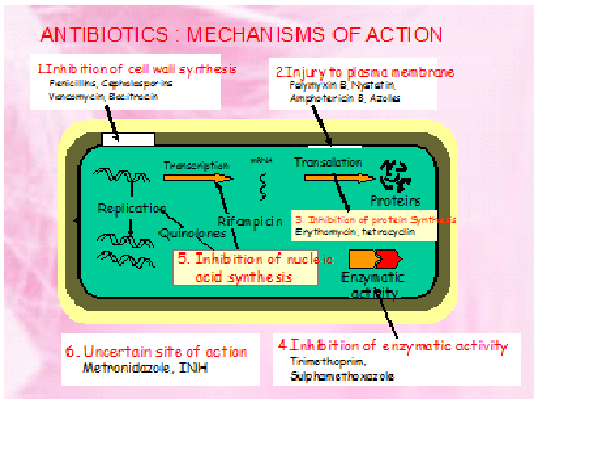
While antibiotics are natural antimicrobial agents produced by microorganisms such as fungi, actinomycetes and bacteria that is capable in small concentrations to kill or inhibit the growth of other bacteria. However, in common usage antibiotic means antibacterial agent, excluding agents with antiviral and antifungal activity (Bauman, 2009b).
It is hard to imagine hospital medicine in the preantibiotic era, indeed many of the great advances of modern medicine and surgery would not have been possible without the ability to rely on antibiotics to cure secondary infections (Mackenzie et al., 2007).
Mechanisms of antibiotic action:
Antibiotics target structures and pathways that are unique and important to bacteria such as cell wall synthesis, cytoplasmic membrane synthesis, protein synthesis, nucleic acid (DNA or RNA) synthesis and intermediary metabolism (McCallum, 2010).
A-Inhibition of cell wall synthesis:
Bacterial cell wall function and structure:
A cell wall maintains cellular integrity by countering the effects of osmosis when the cell is in a hypotonic solution. If the wall is disrupted, it no longer prevents the cell from bursting as water moves into the cell by osmosis (Dmitriev et al., 2005).
The major structural component of a bacterial cell wall is its peptidoglycan layer. Peptidoglycan is a huge macromolecule composed of polysaccharide chains of alternating N-acetylglucosamine (NAG) and N-acetylmuramic acid (NAM) molecules that are cross linked by short peptide chains extending between NAM subunits. To enlarge or divide, a cell must synthesize more peptidoglycan by adding new NAG and NAM subunits to existing NAG-NAM chains, and the new NAM subunits must then be bonded to neighboring NAM subunits (Meroueh et al., 2006).
B-Inhibition of cytoplasmic membrane:
Beneath the cell wall, the cytoplasmic membrane essentially acts as a bag that contains the cytoplasm and controls the passage of chemicals into and out of the cell. Extensive damage to membranes' proteins or phospholipids allows the cellular contents to leak out and if not immediately repaired causes death (Manuselis and Mahon, 2007).
Polymyxin B, polymyxin E (colistin), amphotricin B, imidazoles, triazoles and polyenes exert their actions by altering the bacterial cell membranes. The inhibition of cell membrane function leads to escape of macromolecules from the cell resulting in cell damage or death (Chakraborty, 2009).
Polymyxin is effective against gram-negative bateria, particularly pseudomonas, but because it is toxic to human kidneys it is usually reserved for use against pathogens that are resistant to other antibacterial drugs (Bauman, 2009b).
Daptomycin is a new lipopeptide antibiotic that is rapidly bactericidal by binding to the cell membrane in a calcium dependent manner causing depolarization of bacterial membrane potential. This leads to intracellular potassium release. This agent has been approved for use in the treatment of Staphylococcus aureus blood stream infections and skin and soft tissue infections caused by gram-positive bacteria, particularly those organisms that are highly resistant to β-lactam agents and vancomycin (Brooks and Carroll, 2010).
C-Inhibition of protein synthesis:
Cells use proteins for structure and regulation, as enzymes in metabolism and as channels and pumps to move materials across cell membranes. Thus, a consistent supply of proteins is vital for the active life of a cell (Bauman, 2009a).
Many antimicrobial agents take the advantage of the differences between prokaryotic ribosomes (70S) and the eukaryotic ribosomes (80S) to selectively target bacterial protein translation without significantly affecting eukaryotes (Franceschi and Duffy, 2006).
The 70S ribosome is composed of two subunits 30S and 50S built with RNA and proteins (30S composed of 16S rRNA and ribosomal proteins, 50S subunit composed of 23S rRNA, 5S rRNA and ribosomal proteins) which assemble to produce a functional structure for protein synthesis. Each part undertakes a specific function. The small subunit 30S decodes mRNA. In the large 50S part, the protein is formed by the polymerization of amino acids according to the genetic code. tRNA molecules carry the amino acids. Ribosomes possess three tRNA binding sites A, P, and E, hosting the aminoacyl-tRNA, the peptidyl-tRNA, and the exiting tRNA, respectively. Each elongation cycle involves the advancement of the mRNA together with A→ P → E site passage of the tRNA molecule (Agmon et al., 2004).
Antibiotics that target the 30S ribosomal subunit:
• Aminoglycosides:
The aminoglycosides antibiotics (streptomycin, gentamycin, tobramycin, spectinomycin, kanamycin, neomycin and paromycin) are closely related drugs. They have action against a wide range of micro-organisms (Chakraborty, 2009).
The mode of action of streptomycin has been studied more intensively than other aminoglycosides, but all probably act similarly. The first step is the attachment of the aminoglycoside to a specific receptor protein (S12 in the case of streptomycin) on the 30S subunit of the microbial ribosome. Second, the aminoglycoside blocks the normal activity of the "initiation complex" of peptide formation (mRNA + formyl methionine + tRNA). Third, the mRNA message is misread on the "recognition region" of the ribosome; consequently, the wrong amino acid is inserted into the peptide, resulting in a non functional protein. Fourth, aminoglycoside attachment results in break up of polysomes and their separation into monosomes incapable of protein synthesis (Brooks and Carroll, 2010).
• Tetracyclines:
Tetracyclins bind to the 30S ribosomal subunit and inhibit protein synthesis by blocking the attachment of incoming aminoacyl-tRNA. Thus they prevent introduction of new amino acids to the growing peptide chain (Chopra and Roberts, 2001).
Antibiotics that target the 50S ribosomal subunit:
• Chloramphenicol:
The molecular target for chloramphenicol is the peptidyl transferase enzyme that links amino acids in the growing peptide chain. The effect of the antibiotic is thus to freeze the process of chain elongation, bringing bacterial growth to an abrupt halt. The process is completely reversible, and chloramphenicol is fundamentally a bacteriostatic agent (Biswas et al., 2008).
• Macrolides, Lincosamide and streptogramins :
Macrolides, lincosamides, and streptogramin B (MLSB) antibiotics are structurally dissimilar, but are grouped together due to a common mechanism of action. Macrolides include the drugs erythromycin, clarithromycin, and azithromycin. Clindamycin is the main lincosamide used clinically. Quinupristin, combined with streptogramin A dalfopristin, is the most commonly used streptogramin B antibiotic (Champney and Tober, 2000).
The binding site of these drugs is the 23S of bacterial ribosomal RNA. Binding of the antibiotic prevents movement of the ribosome from one codon to the next; as a result, translation is frozen and protein synthesis is halted (Tsui et al., 2004).
• Oxazolidinones:
The oxazolidinones are a relatively new class of antibiotics. These antibiotics inhibit bacterial growth by interfering with the 50S particle assembly and the binding of aminoacyl-tRNA to the ribosomal A site, as shown for linezolid (Leach et al., 2007).
read more at
Biosafety Recommendations for the Contained Use of M. tuberculosis
The WHO and the CDC classify M. tuberculosis among the pathogens that require a biosafety level 3. Based on the risk assessment and according to technical characteristics, safety equipment and work practices (Philippe et al., 2006).
The following recommendations for the contained use of M. tuberculosis are proposed (CDC, 1999; WHO, Laboratory Safety Manual, 2004):
1) Any containers used for collecting clinical specimens could be contaminated with tubercle bacilli, primary or secondary culture samples or any other material known to contain M. tuberculosis should be opened in a class I or II biosafety cabinet (BSC). Personnel wearing gloves should disinfect the outside of the container.
2) For the laboratory involved in the diagnosis of tuberculosis, direct smear examination and primary culture of specimens require to work in BSL-2 facilities. Primary cultures only concern cultures obtained directly from clinical specimens in solid or liquid culture medium. They should be performed in "unbreakable" vials. These laboratories should send the positive primary culture, without any subsequent examination, to a BSL-3 laboratory for further analysis.
3) When the diagnostic or research laboratory is involved into subsequent characterization of the tubercle bacilli by means of secondary cultures, antimicrobial susceptibility testing, and any other test performed on primary or secondary living cultures, BSL-3 facilities, equipment and work practices should be used.
4) Needle sampling through vial's septum (e.g. for smear examination, nucleic acid amplification or any other biological test) should not be performed.
5) Contaminated pipettes should be discarded horizontally in a container immediately after use. This container must be dry in order to avoid aerosol production pipette laying down.
6) Disposable plastic bacteriological loops are preferable; if wire loops are used, they must be sterilized in an electrically operated “micro-incinerator”. Alternatively, they may be submerged into a flask filled with sand and 90% alcohol, before they are flamed.
7) Needles and syringes or other sharps should be restricted in the laboratory and only used when there is no alternative: only disposable syringe-needle units (i.e., needle are sealed to the syringe) should be used for injection or aspiration of infectious material.
8) Contaminated syringes should be carefully discarded after use in special puncture-resistant containers used for sharps disposal.
9) Appropriate systems of respiratory protection with HEPA filtration should be worn when aerosols cannot be safely contained or for the handling of positive cultures in the BSC.
10) The slides used for AFB smear identification should be handled with care to prevent contamination of hands and discarded after use as potentially contaminated waste.
Smears, which may contain M. tuberculosis, should be stored in a closed box as it was shown that viable tubercle bacilli could be excreted by cockroaches following ingestion from heat-fixed smears (Allen, 1987).
Flow cytometry applications involving M. tuberculosis should take into account recent publications and specific biosafety guidelines (Schmid et al., 2003).
Disinfection, inactivation of M. tuberculosis and waste management
The high lipid content of the cell wall confers to the mycobacteria a great resistance to classical disinfectants. The bacilli are generally more resistant to chemical disinfection than other vegetative bacteria. Their resistance to disinfectants is considered intermediate between other non-sporulating bacteria and spores (Kunz & Gundermann, 1982).
The acquired multidrug resistance does not seem to modify the resistance to disinfectants (Sattar et al., 1995). Quaternary ammoniums inhibit tubercle bacilli but do not kill them. M. tuberculosis is also resistant to acids and alkali. Mercurial compounds are considered to be ineffective against the mycobacteria. Efficient disinfectants are 5% phenol, 5% formaldehyde during at least ten minutes, 2% glutaraldehyde during 30 minutes exposure or sodium hypochlorite (5%) during one minute. Ethyl and isopropyl alcohols in high concentrations are generally accepted to be excellent mycobactericidal agents. 70% ethyl alcohol can be used as surface disinfectant. Formaldehyde vapours can be used to disinfect BSC's and facilities. Iodine and ionophores are considered to be effective against mycobacteria and are generally used in combination with ethyl alcohol (Rubin, 1991).
It is recommended to test killing methods used on M. tuberculosis suspension before removal from Biosafety Level 3 laboratory. A study compared the efficacy of several disinfectant mixtures on class of risk 3 M. tuberculosis Erdman strain. It was observed that fixatives containing low concentration of glutaraldehyde alone are not efficient to kill M. tuberculosis. The use of a combination of 2% paraformaldehyde and 2% glutaraldehyde or a solution of 5% formalin is recommended for M. tuberculosis inactivation (Schwebach et al., 2001). Another experimental study has demonstrated that all tubercle bacilli killing methods should be validated by individual laboratories before removing material derived from M. tuberculosis to the outside of the BSL-3 laboratory (Blackwood et al.,2005).
Work surfaces should be decontaminated at least once a day with an appropriate disinfectant and immediately after any accidental contamination with infectious materials. Laboratory workers should disinfect their hands after manipulations with an appropriate disinfectant, after removing gloves, and before leaving the laboratory. Worn gloves and protecting clothes should be autoclaved before leaving the laboratory (Philippe et al., 2006).
Attention should be given to waste inactivation. Decontamination by autoclaving or incineration is essential. Ideally, an autoclave for the sterilisation of contaminated materials should be available in or adjacent to the laboratory. If the inactivation takes place outside the laboratory (autoclave or incinerator), wastes should be placed in a leak proof bag or an unbreakable and leak proof container (for liquid wastes), sealed and disinfected on the outside before removal from the laboratory. In addition to the international Biohazard symbol, bags or containers should be adequately labelled to prevent opening before decontamination. Removal of bags and containers should be performed according to written procedures. (Kimman et al., 2008b).
Generally, special care should also be taken for the following manipulations (Philippe et al., 2006):
1) Acid-fast staining (AFB smear): smear fixation on slides (by heat or methanol) can generate aerosols. Although fixed smear may still contain viable organisms, they are not easily aerosolized.
2) Manipulation of solid and liquid cultures: Unlike sporulating fungi or bacteria, the opening of a Petri dish or a tube lid containing mycobacteria is not thought to pose a real risk. However, manipulation of the colony mass increases the likelihood of dispersal of the tubercle bacilli into the air, especially when organisms are incinerated from the bacteriological needle or loop. In case of accidental breakage involving culture tubes, a culture of M. tuberculosis grown on a solid medium is rated as producing a “minimal” aerosol requiring local disinfection.
3) flow cytometry: applications of flow cytometry in clinical microbiology and research laboratories are numerous with direct detection of infected cells or isolated mycobacteria, serological tests, monitoring of infections, antimicrobial therapies and cell-sorting
4) In experimental settings, flow cytometry has also been used to assess sputum decontamination methods improvement. Flow cytometry analysis and/or sorting procedures can generate aerosols containing viable M.tuberculosis
The following recommendations for the contained use of M. tuberculosis are proposed (CDC, 1999; WHO, Laboratory Safety Manual, 2004):
1) Any containers used for collecting clinical specimens could be contaminated with tubercle bacilli, primary or secondary culture samples or any other material known to contain M. tuberculosis should be opened in a class I or II biosafety cabinet (BSC). Personnel wearing gloves should disinfect the outside of the container.
2) For the laboratory involved in the diagnosis of tuberculosis, direct smear examination and primary culture of specimens require to work in BSL-2 facilities. Primary cultures only concern cultures obtained directly from clinical specimens in solid or liquid culture medium. They should be performed in "unbreakable" vials. These laboratories should send the positive primary culture, without any subsequent examination, to a BSL-3 laboratory for further analysis.
3) When the diagnostic or research laboratory is involved into subsequent characterization of the tubercle bacilli by means of secondary cultures, antimicrobial susceptibility testing, and any other test performed on primary or secondary living cultures, BSL-3 facilities, equipment and work practices should be used.
4) Needle sampling through vial's septum (e.g. for smear examination, nucleic acid amplification or any other biological test) should not be performed.
5) Contaminated pipettes should be discarded horizontally in a container immediately after use. This container must be dry in order to avoid aerosol production pipette laying down.
6) Disposable plastic bacteriological loops are preferable; if wire loops are used, they must be sterilized in an electrically operated “micro-incinerator”. Alternatively, they may be submerged into a flask filled with sand and 90% alcohol, before they are flamed.
7) Needles and syringes or other sharps should be restricted in the laboratory and only used when there is no alternative: only disposable syringe-needle units (i.e., needle are sealed to the syringe) should be used for injection or aspiration of infectious material.
8) Contaminated syringes should be carefully discarded after use in special puncture-resistant containers used for sharps disposal.
9) Appropriate systems of respiratory protection with HEPA filtration should be worn when aerosols cannot be safely contained or for the handling of positive cultures in the BSC.
10) The slides used for AFB smear identification should be handled with care to prevent contamination of hands and discarded after use as potentially contaminated waste.
Smears, which may contain M. tuberculosis, should be stored in a closed box as it was shown that viable tubercle bacilli could be excreted by cockroaches following ingestion from heat-fixed smears (Allen, 1987).
Flow cytometry applications involving M. tuberculosis should take into account recent publications and specific biosafety guidelines (Schmid et al., 2003).
Disinfection, inactivation of M. tuberculosis and waste management
The high lipid content of the cell wall confers to the mycobacteria a great resistance to classical disinfectants. The bacilli are generally more resistant to chemical disinfection than other vegetative bacteria. Their resistance to disinfectants is considered intermediate between other non-sporulating bacteria and spores (Kunz & Gundermann, 1982).
The acquired multidrug resistance does not seem to modify the resistance to disinfectants (Sattar et al., 1995). Quaternary ammoniums inhibit tubercle bacilli but do not kill them. M. tuberculosis is also resistant to acids and alkali. Mercurial compounds are considered to be ineffective against the mycobacteria. Efficient disinfectants are 5% phenol, 5% formaldehyde during at least ten minutes, 2% glutaraldehyde during 30 minutes exposure or sodium hypochlorite (5%) during one minute. Ethyl and isopropyl alcohols in high concentrations are generally accepted to be excellent mycobactericidal agents. 70% ethyl alcohol can be used as surface disinfectant. Formaldehyde vapours can be used to disinfect BSC's and facilities. Iodine and ionophores are considered to be effective against mycobacteria and are generally used in combination with ethyl alcohol (Rubin, 1991).
It is recommended to test killing methods used on M. tuberculosis suspension before removal from Biosafety Level 3 laboratory. A study compared the efficacy of several disinfectant mixtures on class of risk 3 M. tuberculosis Erdman strain. It was observed that fixatives containing low concentration of glutaraldehyde alone are not efficient to kill M. tuberculosis. The use of a combination of 2% paraformaldehyde and 2% glutaraldehyde or a solution of 5% formalin is recommended for M. tuberculosis inactivation (Schwebach et al., 2001). Another experimental study has demonstrated that all tubercle bacilli killing methods should be validated by individual laboratories before removing material derived from M. tuberculosis to the outside of the BSL-3 laboratory (Blackwood et al.,2005).
Work surfaces should be decontaminated at least once a day with an appropriate disinfectant and immediately after any accidental contamination with infectious materials. Laboratory workers should disinfect their hands after manipulations with an appropriate disinfectant, after removing gloves, and before leaving the laboratory. Worn gloves and protecting clothes should be autoclaved before leaving the laboratory (Philippe et al., 2006).
Attention should be given to waste inactivation. Decontamination by autoclaving or incineration is essential. Ideally, an autoclave for the sterilisation of contaminated materials should be available in or adjacent to the laboratory. If the inactivation takes place outside the laboratory (autoclave or incinerator), wastes should be placed in a leak proof bag or an unbreakable and leak proof container (for liquid wastes), sealed and disinfected on the outside before removal from the laboratory. In addition to the international Biohazard symbol, bags or containers should be adequately labelled to prevent opening before decontamination. Removal of bags and containers should be performed according to written procedures. (Kimman et al., 2008b).
Generally, special care should also be taken for the following manipulations (Philippe et al., 2006):
1) Acid-fast staining (AFB smear): smear fixation on slides (by heat or methanol) can generate aerosols. Although fixed smear may still contain viable organisms, they are not easily aerosolized.
2) Manipulation of solid and liquid cultures: Unlike sporulating fungi or bacteria, the opening of a Petri dish or a tube lid containing mycobacteria is not thought to pose a real risk. However, manipulation of the colony mass increases the likelihood of dispersal of the tubercle bacilli into the air, especially when organisms are incinerated from the bacteriological needle or loop. In case of accidental breakage involving culture tubes, a culture of M. tuberculosis grown on a solid medium is rated as producing a “minimal” aerosol requiring local disinfection.
3) flow cytometry: applications of flow cytometry in clinical microbiology and research laboratories are numerous with direct detection of infected cells or isolated mycobacteria, serological tests, monitoring of infections, antimicrobial therapies and cell-sorting
4) In experimental settings, flow cytometry has also been used to assess sputum decontamination methods improvement. Flow cytometry analysis and/or sorting procedures can generate aerosols containing viable M.tuberculosis
Laboratory design and facilities
In designing a laboratory and assigning certain types of work to it, special attention should be paid to conditions that are known to pose safety problems. These include: 1. Formation of aerosols, 2. Work with large volumes and/or high concentrations of microorganisms, 3. Overcrowding and too much equipment, 4. Infestation with rodents and arthropods, 5. Unauthorized entrance and 6. Workflow: use of specific samples and reagents (Ionescu et al., 2007).
Design features:
For proper design, wide space must be provided for the safe conduct of laboratory work and for cleaning and maintenance. Walls, ceilings and floors should be smooth, easy to clean, impermeable to liquids and resistant to the chemicals and disinfectants normally used in the laboratory. Floors should be slip-resistant. Bench tops should be impervious to water and resistant to disinfectants, acids, alkalis, organic solvents and moderate heat (Stevens, 2003).
Laboratory illumination should be adequate for all activities. Undesirable reflections and glare should be avoided. Laboratory furniture should be sturdy. Open spaces between and under benches, cabinets and equipment should be accessible for cleaning. While Storage space must be adequate to hold supplies for immediate use and thus prevent clutter on bench tops and in aisles. Additional long-term storage space, conveniently located outside the laboratory working areas, should also be provided (Susan and Lauren, 2004).
For proper laboratory design, Space and facilities should be provided for the safe handling and storage of solvents, radioactive materials, and compressed and liquefied gases. Facilities for eating and drinking and for rest should be provided outside the laboratory working areas. Hand-washing basins, with running water if possible, should be provided in each laboratory room, preferably near the exit door. While safety systems should cover fire, electrical emergencies, emergency shower and eyewash facilities and first-aid areas or rooms suitably equipped and readily accessible should be available (Tjeerd et al., 2008).
In the planning of new facilities, consideration should be given to the provision of mechanical ventilation systems that provide an inward flow of air without recirculation. If there is no mechanical ventilation, windows should be able to be opened and should be fitted with arthropod-proof screens. At Biosafety Level 2, an autoclave or other means of decontamination should be available in appropriate proximity to the laboratory (Robert, 2007).
Code of practice
This code is a listing of the most essential laboratory practices and procedures that are basic to GMT. In many laboratories and national laboratory programmes, this code may be used to develop written practices and procedures for safe laboratory operations (Ezzelle, et al., 2008).
Personal protection
Laboratory personelles protection can be fulfilled by coveralls, gowns or uniforms must be worn at all times for work in the laboratory. Appropriate gloves must be worn for all procedures that may involve direct or accidental contact with blood, body fluids and other potentially infectious materials or infected animals. After use, gloves should be removed and hands must then be washed (David, 2003).
For proper safety, personnel must wash their hands after handling infectious materials and animals, and before they leave the laboratory working areas. Safety glasses, face shields (visors) or other protective devices must be worn when it is necessary to protect the eyes and face from splashes, impacting objects and sources of artificial ultraviolet radiation (Ezzelle, et al., 2008).
Procedures
For GMT, Pipetting by mouth must be strictly forbidden. Materials must not be placed in the mouth. Labels must not be licked. All technical procedures should be performed in a way that minimizes the formation of aerosols and droplets. The use of hypodermic needles and syringes should be limited. They must not be used as substitutes for pipetting devices or for any purpose other than parenteral injection or aspiration of fluids from laboratory animals (Stevens, 2003).
Also, all spills, accidents and overt or potential exposures to infectious materials must be reported to the laboratory supervisor. A written record of such accidents and incidents should be maintained. A written procedure for the clean-up of all spills must be developed and followed. Contaminated liquids must be decontaminated (chemically or physically) before discharge to the sanitary sewer. An effluent treatment system may be required, depending on the risk assessment for the agent(s) being handled (Ionescu et al., 2007).
Laboratory working areas
The laboratory should be kept neat, clean and free of materials that are not pertinent to the work. Work surfaces must be decontaminated after any spill of potentially dangerous material and at the end of the working day. All contaminated materials, specimens and cultures must be decontaminated before disposal or cleaning for reuse. Packing and transportation must follow applicable national and/or international regulations. When windows can be opened, they should be fitted with arthropod-proof screens (Ricós et al., 2008).
Biosafety management
Biosafety management is the responsibility of the laboratory director (the person who has immediate responsibility for the laboratory) to ensure the development and adoption of a biosafety management plan and a safety or operations manual. The laboratory supervisor (reporting to the laboratory director) should ensure that regular training in laboratory safety is provided (Ionescu et al., 2007).
Laboratory equipment
Together with good procedures and practices, the use of safety equipment will help to reduce risks when dealing with biosafety hazards. This section deals with basic principles related to equipment suitable for laboratories of all biosafety levels.The laboratory director should, after consultation with the biosafety officer and safety committee (if designated), ensure that adequate equipment is provided and that it is used properly. Equipment should be selected to take account of certain general principles, i.e. it should be designed to prevent or limit contact between the operator and the infectious material. Also, it should be constructed of materials that are impermeable to liquids, resistant to corrosion and meet structural requirements and fabricated to be free of burrs, sharp edges and unguarded moving parts (Ezzelle, et al., 2008).
Essential biosafety equipment
Essential biosafety equipments include pipetting aids to avoid mouth pipetting. Many different designs are available. Also, biological safety cabinets should be used whenever infectious materials are handled specially with procedures with a high potential for producing aerosols; these may include centrifugation, grinding, blending, vigorous shaking or mixing, sonic disruption, opening of containers of infectious materials whose internal pressure may be different from the ambient pressure, intranasal inoculation of animals, and harvesting of infectious tissues from animals and eggs (Kimman et al., 2008a).
Plastic disposable transfer loops also should be available. Alternatively, electric transfer loop incinerators may be used inside the biological safety cabinet to reduce aerosol production. Screw-capped tubes and bottles, autoclaves or other appropriate means to decontaminate infectious materials are also required (Kimman et al., 2008b).
Waste handling
Waste is anything that is to be discarded. In laboratories, decontamination of wastes and their ultimate disposal are closely interrelated. In terms of daily use, few if any contaminated materials will require actual removal from the laboratory or destruction. Most glassware, instruments and laboratory clothing will be reused or recycled. The overriding principle is that all infectious materials should be decontaminated, autoclaved or incinerated within the laboratory (Shahangian and Snyder, 2009)
Design features:
For proper design, wide space must be provided for the safe conduct of laboratory work and for cleaning and maintenance. Walls, ceilings and floors should be smooth, easy to clean, impermeable to liquids and resistant to the chemicals and disinfectants normally used in the laboratory. Floors should be slip-resistant. Bench tops should be impervious to water and resistant to disinfectants, acids, alkalis, organic solvents and moderate heat (Stevens, 2003).
Laboratory illumination should be adequate for all activities. Undesirable reflections and glare should be avoided. Laboratory furniture should be sturdy. Open spaces between and under benches, cabinets and equipment should be accessible for cleaning. While Storage space must be adequate to hold supplies for immediate use and thus prevent clutter on bench tops and in aisles. Additional long-term storage space, conveniently located outside the laboratory working areas, should also be provided (Susan and Lauren, 2004).
For proper laboratory design, Space and facilities should be provided for the safe handling and storage of solvents, radioactive materials, and compressed and liquefied gases. Facilities for eating and drinking and for rest should be provided outside the laboratory working areas. Hand-washing basins, with running water if possible, should be provided in each laboratory room, preferably near the exit door. While safety systems should cover fire, electrical emergencies, emergency shower and eyewash facilities and first-aid areas or rooms suitably equipped and readily accessible should be available (Tjeerd et al., 2008).
In the planning of new facilities, consideration should be given to the provision of mechanical ventilation systems that provide an inward flow of air without recirculation. If there is no mechanical ventilation, windows should be able to be opened and should be fitted with arthropod-proof screens. At Biosafety Level 2, an autoclave or other means of decontamination should be available in appropriate proximity to the laboratory (Robert, 2007).
Code of practice
This code is a listing of the most essential laboratory practices and procedures that are basic to GMT. In many laboratories and national laboratory programmes, this code may be used to develop written practices and procedures for safe laboratory operations (Ezzelle, et al., 2008).
Personal protection
Laboratory personelles protection can be fulfilled by coveralls, gowns or uniforms must be worn at all times for work in the laboratory. Appropriate gloves must be worn for all procedures that may involve direct or accidental contact with blood, body fluids and other potentially infectious materials or infected animals. After use, gloves should be removed and hands must then be washed (David, 2003).
For proper safety, personnel must wash their hands after handling infectious materials and animals, and before they leave the laboratory working areas. Safety glasses, face shields (visors) or other protective devices must be worn when it is necessary to protect the eyes and face from splashes, impacting objects and sources of artificial ultraviolet radiation (Ezzelle, et al., 2008).
Procedures
For GMT, Pipetting by mouth must be strictly forbidden. Materials must not be placed in the mouth. Labels must not be licked. All technical procedures should be performed in a way that minimizes the formation of aerosols and droplets. The use of hypodermic needles and syringes should be limited. They must not be used as substitutes for pipetting devices or for any purpose other than parenteral injection or aspiration of fluids from laboratory animals (Stevens, 2003).
Also, all spills, accidents and overt or potential exposures to infectious materials must be reported to the laboratory supervisor. A written record of such accidents and incidents should be maintained. A written procedure for the clean-up of all spills must be developed and followed. Contaminated liquids must be decontaminated (chemically or physically) before discharge to the sanitary sewer. An effluent treatment system may be required, depending on the risk assessment for the agent(s) being handled (Ionescu et al., 2007).
Laboratory working areas
The laboratory should be kept neat, clean and free of materials that are not pertinent to the work. Work surfaces must be decontaminated after any spill of potentially dangerous material and at the end of the working day. All contaminated materials, specimens and cultures must be decontaminated before disposal or cleaning for reuse. Packing and transportation must follow applicable national and/or international regulations. When windows can be opened, they should be fitted with arthropod-proof screens (Ricós et al., 2008).
Biosafety management
Biosafety management is the responsibility of the laboratory director (the person who has immediate responsibility for the laboratory) to ensure the development and adoption of a biosafety management plan and a safety or operations manual. The laboratory supervisor (reporting to the laboratory director) should ensure that regular training in laboratory safety is provided (Ionescu et al., 2007).
Laboratory equipment
Together with good procedures and practices, the use of safety equipment will help to reduce risks when dealing with biosafety hazards. This section deals with basic principles related to equipment suitable for laboratories of all biosafety levels.The laboratory director should, after consultation with the biosafety officer and safety committee (if designated), ensure that adequate equipment is provided and that it is used properly. Equipment should be selected to take account of certain general principles, i.e. it should be designed to prevent or limit contact between the operator and the infectious material. Also, it should be constructed of materials that are impermeable to liquids, resistant to corrosion and meet structural requirements and fabricated to be free of burrs, sharp edges and unguarded moving parts (Ezzelle, et al., 2008).
Essential biosafety equipment
Essential biosafety equipments include pipetting aids to avoid mouth pipetting. Many different designs are available. Also, biological safety cabinets should be used whenever infectious materials are handled specially with procedures with a high potential for producing aerosols; these may include centrifugation, grinding, blending, vigorous shaking or mixing, sonic disruption, opening of containers of infectious materials whose internal pressure may be different from the ambient pressure, intranasal inoculation of animals, and harvesting of infectious tissues from animals and eggs (Kimman et al., 2008a).
Plastic disposable transfer loops also should be available. Alternatively, electric transfer loop incinerators may be used inside the biological safety cabinet to reduce aerosol production. Screw-capped tubes and bottles, autoclaves or other appropriate means to decontaminate infectious materials are also required (Kimman et al., 2008b).
Waste handling
Waste is anything that is to be discarded. In laboratories, decontamination of wastes and their ultimate disposal are closely interrelated. In terms of daily use, few if any contaminated materials will require actual removal from the laboratory or destruction. Most glassware, instruments and laboratory clothing will be reused or recycled. The overriding principle is that all infectious materials should be decontaminated, autoclaved or incinerated within the laboratory (Shahangian and Snyder, 2009)
Laboratory design and facilities
In designing a laboratory and assigning certain types of work to it, special attention should be paid to conditions that are known to pose safety problems. These include: 1. Formation of aerosols, 2. Work with large volumes and/or high concentrations of microorganisms, 3. Overcrowding and too much equipment, 4. Infestation with rodents and arthropods, 5. Unauthorized entrance and 6. Workflow: use of specific samples and reagents (Ionescu et al., 2007).
Design features:
For proper design, wide space must be provided for the safe conduct of laboratory work and for cleaning and maintenance. Walls, ceilings and floors should be smooth, easy to clean, impermeable to liquids and resistant to the chemicals and disinfectants normally used in the laboratory. Floors should be slip-resistant. Bench tops should be impervious to water and resistant to disinfectants, acids, alkalis, organic solvents and moderate heat (Stevens, 2003).
Laboratory illumination should be adequate for all activities. Undesirable reflections and glare should be avoided. Laboratory furniture should be sturdy. Open spaces between and under benches, cabinets and equipment should be accessible for cleaning. While Storage space must be adequate to hold supplies for immediate use and thus prevent clutter on bench tops and in aisles. Additional long-term storage space, conveniently located outside the laboratory working areas, should also be provided (Susan and Lauren, 2004).
For proper laboratory design, Space and facilities should be provided for the safe handling and storage of solvents, radioactive materials, and compressed and liquefied gases. Facilities for eating and drinking and for rest should be provided outside the laboratory working areas. Hand-washing basins, with running water if possible, should be provided in each laboratory room, preferably near the exit door. While safety systems should cover fire, electrical emergencies, emergency shower and eyewash facilities and first-aid areas or rooms suitably equipped and readily accessible should be available (Tjeerd et al., 2008).
In the planning of new facilities, consideration should be given to the provision of mechanical ventilation systems that provide an inward flow of air without recirculation. If there is no mechanical ventilation, windows should be able to be opened and should be fitted with arthropod-proof screens. At Biosafety Level 2, an autoclave or other means of decontamination should be available in appropriate proximity to the laboratory (Robert, 2007).
Code of practice
This code is a listing of the most essential laboratory practices and procedures that are basic to GMT. In many laboratories and national laboratory programmes, this code may be used to develop written practices and procedures for safe laboratory operations (Ezzelle, et al., 2008).
Personal protection
Laboratory personelles protection can be fulfilled by coveralls, gowns or uniforms must be worn at all times for work in the laboratory. Appropriate gloves must be worn for all procedures that may involve direct or accidental contact with blood, body fluids and other potentially infectious materials or infected animals. After use, gloves should be removed and hands must then be washed (David, 2003).
For proper safety, personnel must wash their hands after handling infectious materials and animals, and before they leave the laboratory working areas. Safety glasses, face shields (visors) or other protective devices must be worn when it is necessary to protect the eyes and face from splashes, impacting objects and sources of artificial ultraviolet radiation (Ezzelle, et al., 2008).
Procedures
For GMT, Pipetting by mouth must be strictly forbidden. Materials must not be placed in the mouth. Labels must not be licked. All technical procedures should be performed in a way that minimizes the formation of aerosols and droplets. The use of hypodermic needles and syringes should be limited. They must not be used as substitutes for pipetting devices or for any purpose other than parenteral injection or aspiration of fluids from laboratory animals (Stevens, 2003).
Also, all spills, accidents and overt or potential exposures to infectious materials must be reported to the laboratory supervisor. A written record of such accidents and incidents should be maintained. A written procedure for the clean-up of all spills must be developed and followed. Contaminated liquids must be decontaminated (chemically or physically) before discharge to the sanitary sewer. An effluent treatment system may be required, depending on the risk assessment for the agent(s) being handled (Ionescu et al., 2007).
Laboratory working areas
The laboratory should be kept neat, clean and free of materials that are not pertinent to the work. Work surfaces must be decontaminated after any spill of potentially dangerous material and at the end of the working day. All contaminated materials, specimens and cultures must be decontaminated before disposal or cleaning for reuse. Packing and transportation must follow applicable national and/or international regulations. When windows can be opened, they should be fitted with arthropod-proof screens (Ricós et al., 2008).
Biosafety management
Biosafety management is the responsibility of the laboratory director (the person who has immediate responsibility for the laboratory) to ensure the development and adoption of a biosafety management plan and a safety or operations manual. The laboratory supervisor (reporting to the laboratory director) should ensure that regular training in laboratory safety is provided (Ionescu et al., 2007).
Laboratory equipment
Together with good procedures and practices, the use of safety equipment will help to reduce risks when dealing with biosafety hazards. This section deals with basic principles related to equipment suitable for laboratories of all biosafety levels.The laboratory director should, after consultation with the biosafety officer and safety committee (if designated), ensure that adequate equipment is provided and that it is used properly. Equipment should be selected to take account of certain general principles, i.e. it should be designed to prevent or limit contact between the operator and the infectious material. Also, it should be constructed of materials that are impermeable to liquids, resistant to corrosion and meet structural requirements and fabricated to be free of burrs, sharp edges and unguarded moving parts (Ezzelle, et al., 2008).
Essential biosafety equipment
Essential biosafety equipments include pipetting aids to avoid mouth pipetting. Many different designs are available. Also, biological safety cabinets should be used whenever infectious materials are handled specially with procedures with a high potential for producing aerosols; these may include centrifugation, grinding, blending, vigorous shaking or mixing, sonic disruption, opening of containers of infectious materials whose internal pressure may be different from the ambient pressure, intranasal inoculation of animals, and harvesting of infectious tissues from animals and eggs (Kimman et al., 2008a).
Plastic disposable transfer loops also should be available. Alternatively, electric transfer loop incinerators may be used inside the biological safety cabinet to reduce aerosol production. Screw-capped tubes and bottles, autoclaves or other appropriate means to decontaminate infectious materials are also required (Kimman et al., 2008b).
Waste handling
Waste is anything that is to be discarded. In laboratories, decontamination of wastes and their ultimate disposal are closely interrelated. In terms of daily use, few if any contaminated materials will require actual removal from the laboratory or destruction. Most glassware, instruments and laboratory clothing will be reused or recycled. The overriding principle is that all infectious materials should be decontaminated, autoclaved or incinerated within the laboratory (Shahangian and Snyder, 2009)
Design features:
For proper design, wide space must be provided for the safe conduct of laboratory work and for cleaning and maintenance. Walls, ceilings and floors should be smooth, easy to clean, impermeable to liquids and resistant to the chemicals and disinfectants normally used in the laboratory. Floors should be slip-resistant. Bench tops should be impervious to water and resistant to disinfectants, acids, alkalis, organic solvents and moderate heat (Stevens, 2003).
Laboratory illumination should be adequate for all activities. Undesirable reflections and glare should be avoided. Laboratory furniture should be sturdy. Open spaces between and under benches, cabinets and equipment should be accessible for cleaning. While Storage space must be adequate to hold supplies for immediate use and thus prevent clutter on bench tops and in aisles. Additional long-term storage space, conveniently located outside the laboratory working areas, should also be provided (Susan and Lauren, 2004).
For proper laboratory design, Space and facilities should be provided for the safe handling and storage of solvents, radioactive materials, and compressed and liquefied gases. Facilities for eating and drinking and for rest should be provided outside the laboratory working areas. Hand-washing basins, with running water if possible, should be provided in each laboratory room, preferably near the exit door. While safety systems should cover fire, electrical emergencies, emergency shower and eyewash facilities and first-aid areas or rooms suitably equipped and readily accessible should be available (Tjeerd et al., 2008).
In the planning of new facilities, consideration should be given to the provision of mechanical ventilation systems that provide an inward flow of air without recirculation. If there is no mechanical ventilation, windows should be able to be opened and should be fitted with arthropod-proof screens. At Biosafety Level 2, an autoclave or other means of decontamination should be available in appropriate proximity to the laboratory (Robert, 2007).
Code of practice
This code is a listing of the most essential laboratory practices and procedures that are basic to GMT. In many laboratories and national laboratory programmes, this code may be used to develop written practices and procedures for safe laboratory operations (Ezzelle, et al., 2008).
Personal protection
Laboratory personelles protection can be fulfilled by coveralls, gowns or uniforms must be worn at all times for work in the laboratory. Appropriate gloves must be worn for all procedures that may involve direct or accidental contact with blood, body fluids and other potentially infectious materials or infected animals. After use, gloves should be removed and hands must then be washed (David, 2003).
For proper safety, personnel must wash their hands after handling infectious materials and animals, and before they leave the laboratory working areas. Safety glasses, face shields (visors) or other protective devices must be worn when it is necessary to protect the eyes and face from splashes, impacting objects and sources of artificial ultraviolet radiation (Ezzelle, et al., 2008).
Procedures
For GMT, Pipetting by mouth must be strictly forbidden. Materials must not be placed in the mouth. Labels must not be licked. All technical procedures should be performed in a way that minimizes the formation of aerosols and droplets. The use of hypodermic needles and syringes should be limited. They must not be used as substitutes for pipetting devices or for any purpose other than parenteral injection or aspiration of fluids from laboratory animals (Stevens, 2003).
Also, all spills, accidents and overt or potential exposures to infectious materials must be reported to the laboratory supervisor. A written record of such accidents and incidents should be maintained. A written procedure for the clean-up of all spills must be developed and followed. Contaminated liquids must be decontaminated (chemically or physically) before discharge to the sanitary sewer. An effluent treatment system may be required, depending on the risk assessment for the agent(s) being handled (Ionescu et al., 2007).
Laboratory working areas
The laboratory should be kept neat, clean and free of materials that are not pertinent to the work. Work surfaces must be decontaminated after any spill of potentially dangerous material and at the end of the working day. All contaminated materials, specimens and cultures must be decontaminated before disposal or cleaning for reuse. Packing and transportation must follow applicable national and/or international regulations. When windows can be opened, they should be fitted with arthropod-proof screens (Ricós et al., 2008).
Biosafety management
Biosafety management is the responsibility of the laboratory director (the person who has immediate responsibility for the laboratory) to ensure the development and adoption of a biosafety management plan and a safety or operations manual. The laboratory supervisor (reporting to the laboratory director) should ensure that regular training in laboratory safety is provided (Ionescu et al., 2007).
Laboratory equipment
Together with good procedures and practices, the use of safety equipment will help to reduce risks when dealing with biosafety hazards. This section deals with basic principles related to equipment suitable for laboratories of all biosafety levels.The laboratory director should, after consultation with the biosafety officer and safety committee (if designated), ensure that adequate equipment is provided and that it is used properly. Equipment should be selected to take account of certain general principles, i.e. it should be designed to prevent or limit contact between the operator and the infectious material. Also, it should be constructed of materials that are impermeable to liquids, resistant to corrosion and meet structural requirements and fabricated to be free of burrs, sharp edges and unguarded moving parts (Ezzelle, et al., 2008).
Essential biosafety equipment
Essential biosafety equipments include pipetting aids to avoid mouth pipetting. Many different designs are available. Also, biological safety cabinets should be used whenever infectious materials are handled specially with procedures with a high potential for producing aerosols; these may include centrifugation, grinding, blending, vigorous shaking or mixing, sonic disruption, opening of containers of infectious materials whose internal pressure may be different from the ambient pressure, intranasal inoculation of animals, and harvesting of infectious tissues from animals and eggs (Kimman et al., 2008a).
Plastic disposable transfer loops also should be available. Alternatively, electric transfer loop incinerators may be used inside the biological safety cabinet to reduce aerosol production. Screw-capped tubes and bottles, autoclaves or other appropriate means to decontaminate infectious materials are also required (Kimman et al., 2008b).
Waste handling
Waste is anything that is to be discarded. In laboratories, decontamination of wastes and their ultimate disposal are closely interrelated. In terms of daily use, few if any contaminated materials will require actual removal from the laboratory or destruction. Most glassware, instruments and laboratory clothing will be reused or recycled. The overriding principle is that all infectious materials should be decontaminated, autoclaved or incinerated within the laboratory (Shahangian and Snyder, 2009)
Subscribe to:
Posts (Atom)